Intensive therapy and progression to clinical albuminuria in patients with insulin dependent diabetes mellitus and microalbuminuria
BMJ 1995; 311 doi: https://doi.org/10.1136/bmj.311.7011.973 (Published 14 October 1995) Cite this as: BMJ 1995;311:973
- Microalbuminuria Collaborative Study Groupa
- Correspondence to: Professor G C Viberti, Unit for Metabolic Medicine, United Medical and Dental Schools of Guy's and St Thomas's Hospitals, London SE1 9RT.
- Accepted 20 August 1995
Abstract
Abstract Objective: To study the effect of intensive therapy of diabetes on the progressio to clinical albuminuria in insulin dependent diabetic patients with microalbuminuria.
Design: Randomised controlled clinical trial of intensive versus conventional therapy ofdiabetes for a median of 5 years (range 2-8).
Setting: Nine hospital based specialist diabetes centres in England and Wales.
Subjects: 70 European insulin dependent diabetic patients aged 17-59 years with microalbuminuria (albumin excretion 30-199 µg/min), but without arterial hypertension, recruited from the nine hospital based specialist diabetes centres.
Interventions: Intensive diabetic therapy was allocated to 36 patients (27 men, 9 women) and conventional diabetic therapy to 34 (24 men, 10 women).
Main outcome measures: Development of clinical albuminuria, defined as albumin excretion greater than 200 µg/min on at least two consecutive occasions, and rate of change of albumin excretion.
Results: Mean glycated haemoglobin concentration, similar at baseline in the two groups (intensive therapy group 10.3% (SEM 1.9%), conventional therapy group 9.8% (1.6%)), fell significantly (by 14%) in the intensive therapy group only. A significant glycaemic separation between the two groups was maintained for up to three years. Progression to clinical albuminuria occurred in six patients in each group. Blood pressure, similar at baseline, fell significantly by 1 mm Hg (95% confidence interval −4.20 to 1.43) per year in the conventional therapy group, but the difference in the rate of blood pressure change between the groups was not significant. Independent of treatment assignment, a mean blood pressure above the group mean (93.6 mm Hg), but not the glycated haemoglobin concentration, predicted progression to clinical albuminuria (relative risk 4.2, 95% confidence interval 1.3 to 13.0).
Conclusions: Intensive therapy with improved glycaemic control for three years had no impact on the progression of albuminuria in insulin dependent diabetic patients with microalbuminuria. The reduction in blood pressure in the conventional therapy group may have affected outcome--in that arterial blood pressure rather than glycated haemoglobin concentration seemed to be the main predictor of progression from microalbuminuria to clinical albuminuria.
Key messages
Key messages
Intensive therapy of diabetes fails to affect the progression of nephropathy in insulin dependent diabetes complicated by microalbuminuria
Blood pressure and not hyperglycaemia is the main determinant of progressive renal disease in these patients
From a therapeutic stand point, preventing the progression of renal disease is better achieved by non-glycaemic interventions such as reducing the blood pressure and treatment with angiotensin converting enzyme inhibitors
Intensive diabetic therapy may improve the course of other complications, such as retinopathy or neuropathy
Introduction
Insulin dependent diabetic patients with poor glycaemic control develop kidney disease more frequently.1 2 3 However, proof that strict blood glucose control reduces the risk of renal complications can come only from prospective intervention studies of intensive therapy of diabetes. Intensive treatment of insulin dependent diabetes mellitus prevents the development of microalbuminuria and clinical albuminuria in patients with baseline normal albumin excretion.4 It is less clear whether progression from microalbuminuria to clinical albuminuria--the hallmark of diabetic nephropathy--can be affected significantly by intensive treatment.
In early studies tight blood glucose control reduced albumin excretion in insulin dependent diabetes mellitus complicated by microalbuminuria, but the studies were too short to examine progression to clinical albuminuria.5 6 In one study clinical albuminuria could be averted, but in another (in patients with insulin dependent diabetes mellitus and intermittent proteinuria) there was no beneficial effect of insulin pump induced strict blood glucose control on either albumin excretion or the rate of decline in the glomerular filtration rate.7 8
The Microalbuminuria Collaborative Study Group was set up in 1984 to screen an unselected outpatient group of insulin dependent diabetic patients for microalbuminuria.9 The aim was to recruit patients into an intervention study of intensive therapy versus conventional therapy and to examine factors which affect progression from normoalbuminuria to microalbuminuria.10 We report the effects of intensive therapy versus conventional therapy on the progression to clinical albuminuria in a group of 70 insulin dependent diabetic patients with microalbuminuria.
Patients and methods
Insulin dependent diabetic patients attending nine hospital based specialist diabetes centres and aged 16-60, with onset of diabetes before the age of 39, no albuminuria by dipstick test, a sitting blood pressure below 160/95 mm Hg, no antihypertensive treatment, and no clinical evidence ofcardiovascular, peripheral vascular, or renal disease were screened for their albumin excretion rate.
Screening procedures and prevalence rates of microalbuminuria were as reported.9 In brief, patients with an albumin concentration >/=15 mg/l or an albumin to creatinine ratio >/=3.5 mg:mmol in a first morning urine sample were asked to provide twotimed overnight urine collections for determination of the albumin excretion rate. Patients whose albumin excretion was greater than 30 µg/min but less than 200 µg/min in at least one of the two samples were recruited. Seventy eligible patients gave written informed consent to the study, whichwas approved by the ethics committee of each participating centre. Patients--all of European origin--were stratified by age and sex and randomised to either intensive therapy or conventional therapy by a centralised procedure.
ASSESSMENT, TREATMENT, AND OUTCOME MEASURES
Patients were assessed at baseline and every three months for two to eight years (median 5.0 years) until the study was closed in September 1993. Patients allocated to intensive therapy received insulin by continuous subcutaneous infusion or by multiple daily injections. They were seen frequently and clear glycaemic targets were set. These were a glycated haemoglobin concentration </=7.5% (normal 4.8-7.5%), a fasting blood glucose concentration between 4 and 6 mmol/l, and a two hour postprandial blood glucose concentration </=10 mmol/l. They performed regular seven point blood glucose profiles and adjusted their treatment regimen in consultation with the investigation team, which was available for advice 24 hours a day.
Except for nine patients who were having more than two insulin injections a day before randomisation, patients allocated to conventional therapy received two daily injections of insulin, including intermediate and short acting insulin. Conventional education about diet, exercise, and self monitoring of blood glucose values was given but targets were not set. The insulin dose and regimen were not adjusted unless the patients became symptomatic. Conventional education about diet, exercise, and self monitoring of blood glucose values was given but targets were not seen. No planned changes were made to the usual diabetic diet of any patient.
At each visit a medical history was taken, including a record of severe episodes of hypoglycaemia or ketoacidosis (that is, which required the assistance of another person), and a full physical examination performed. Patients were classified as smokers if they currently smoked or had stopped for less than a year. Arterial blood pressure (phase I and V) was measured with the patient sitting and after 10 minutes' rest by a random zero sphygmomanometer with appropriately sized cuff. Two readings were recorded to the nearest 2 mm Hg and the average used for calculation. Mean arterial pressure was calculated as diastolic pressure plus one third of the pulse pressure. If the bloodpressure was 160/95 mm Hg or higher at a regular three monthly visit and this was confirmed within a week the attending physician instituted treatment to lower and maintain the blood pressure below this value.
A blood sample was drawn for measurement of glycated haemoglobin concentration (by electroendosmosis; Corning method, Ciba Corning, Halstead, Essex) and serum creatinine concentration (reaction rate method; Hitachi autoanalyser, Boehringer, Lewes, Sussex). These measurements were done in four participating centres (Guy's Hospital; Poole General Hospital; Royal Victoria Infirmary, Newcastle upon Tyne; and Cardiff Royal Infirmary) that regularly exchanged quality control samples and cross validated results.
Timed overnight urine specimens were collected for analysis of albumin concentration by radioimmunoassay6 and creatinine concentration by the Jaffe reaction, which was carried out within seven days in urine stored at 4°C at the central laboratory at Guy's Hospital. Albumin excretion rate was calculated as albumin concentration times urine flow. Glomerular filtration rate was measured within two years of entry into the study and at the end of the study in all patients. The rate was measured by clearance of chromium-51 labelled EDTA11 in 32 intensive therapy patients and 30 conventional therapy patients and by clearance of technetium-99 labelled DTPA12 in four intensive therapy patients and four conventional therapy patients. Thirty one patients had their glomerular filtration rate measured between three and five times.
Funduscopy through dilated pupils was performed every six months and retinal appearances gradedaccording to the scoring system used in the WHO multinational study of vascular disease in diabetes.13
Primary outcome variables were progression to clinical albuminuria, defined as albumin excretion >/=200 µg/min at two consecutive visits, and rate of change in albumin excretion rate.
STATISTICAL METHODS
Data were analysed on an intention to treat basis. The significance of differences was evaluated by the Mann-Whitney test. Time to progression curves were calculated by the method of Kaplan andMeier and significance analysed by log rank test. Cox's proportional hazards model was used to evaluate the significance of continuous baseline variables on time to progression.
To plot mean changes in relevant variables allowance was made for different durations of follow up in different patients and the mean absolute difference between successive values calculated for all patients having values at both time points. These mean differences were cumulated over the entire study and 95% confidence intervals calculated.
To test for differences in rates of change of variables a linear regression was calculated for each variable for each patient and the slopes of these regression lines compared within groups by the Wilcoxon matched pairs signed rank test. Comparison of slopes between groups used weighted linear regression, where the slope represented the dependent variable and the group the predictor variable. Values for albumin excretion were log transformed before analysis. A P value of <0.05 was taken as significant. SAS/STAT software version 6.09 was used for data processing.
Results
The 70 patients were followed up for a median of 5.0 years (range 2 to 8), giving a total of 346 patient years of observation. Thirty six patients were randomised to intensive therapy and 34 toconventional therapy. All but eight patients (five in the intensive therapy group, three in the conventional therapy group) completed the study. Reasons for withdrawal were acute renal failure (one patient), unwillingness to continue (four), moved away (one), developed leukaemia (one), and death (one). Sex distribution, age, body mass index, duration of diabetes, insulin dose, smoking habits, baseline albumin excretion rate, arterial blood pressure, and serum creatinine and glycated haemoglobin concentrations were similar in the two groups but glomerular filtration rate was higher in the intensive therapy group (tables I and II).
Baseline demographic and clinical characteristics of insulin dependent diabetic patients with microalbuminuria
Baseline clinical and biochemical characteristics of insulin dependent diabetic patients with microalbuminuria. Except where stated otherwise, results are means and 95% confidence intervals
Fifty three patients (76%) remained in their assigned groups, nine assigned to conventional therapy changing to multiple injections and eight assigned to intensive therapy reverting to two injections a day. On average, patients received their assigned therapy for 92% of the time that they were in the study.
METABOLIC CONTROL
Glycated haemoglobin concentration fell significantly in the intensive therapy group and reached a nadir after six months (mean 10.3% (SEM 1.9%) versus 8.9% (1.5%); P<0.001), a mean drop of 14%. Glycated haemoglobin concentrations in the conventional therapy group remained unchanged throughout. A significant difference in mean absolute glycated haemoglobin changes from baseline was maintained between the intensive therapy and conventional therapy groups for up to 36 months (P<0.05) (fig 1).

Mean cumulative absolute changes in haemoglobin A1 concentration in insulin dependent diabetic patients with microalbuminuria receiving intensive therapy (closed circles, thick solid line) and conventional therapy (open circles, thin solid line). Bars are 95% confidence intervals
{kind=link}
PERSISTENT ALBUMINURIA
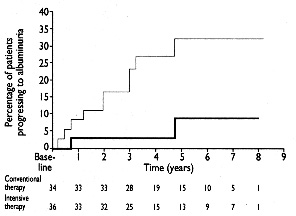
Six patients in each treatment group progressed to clinical albuminuria. The probability of progression was not significantly different between the groups (fig 2). This was the case even when analysis was confined to the first 36 months of the study. The 95% confidence intervals on the mean change in albumin excretion rate, calculated on the slopes of regression, ranged from a decrease of 12.4 µg/min to an increase of 18.4 µg/min during the first five years of follow up. The rates of change in albumin excretion were not significantly different between the groups (P=0.31) even after adjustment for the potential confounding influence of imbalances in baseline values of albumin excretion, blood pressure, and haemoglobin A1 value. Smoking was unrelated to progression.

Cumulative incidence of clinical albuminuria in insulin dependent diabetic patients with microalbuminuria receiving intensive therapy (thick solid line) and conventional therapy (thin solid line)
{kind=link}
Arterial pressure was similar in the two groups at baseline but subsequently declined significantly in the conventional therapy group only--by an average of 1.0 mm Hg yearly (95% confidence interval −4.2 to 1.4; P=0.005) (fig 3). The difference in blood pressure slopes between the two groups, however, was not significant (P=0.29). Five intensive therapy and four conventional therapy patients developed arterial hypertension (that is, blood pressure >/=160/95 mm Hg) and received similar antihypertensive treatment, which included angiotensin converting enzyme inhibitors, ß blockers, calcium antagonists, and loop diuretics either singly or in combination.

Mean cumulative absolute changes in mean blood pressure in insulin dependent diabetic patients with microalbuminuria receiving intensive therapy (closed circles, thick solid line) and conventional therapy (open circles, thin solid line). Bars are 95% confidence intervals
{kind=link}
End of study glomerular filtration rates (mean and 95% confidence intervals) were similar in the two groups (intensive therapy group 100 (90 to 110) ml/min/1.73 m2, conventional therapy group 108 (98 to 118) ml/min/1.73 m2). In the intensive therapy group the glomerular filtration rate was significantly higher at baseline (table II) and fell significantly (P<0.001), possibly because of improved blood glucose control.14 Renal failure (glomerular filtration rate 17 ml/min/1.73 m2) developed in one intensive therapy patient, while moderate renal impairment occurred in another intensive therapy patient (glomerular filtration rate 42 ml/min/1.73 m2) and in two conventional therapy patients (48 and 54 ml/min/1.73 m2).
In the whole group of patients those with mean arterial pressure above the group mean (93.6 mm Hg) had a significantly higher probability (relative risk 4.2 (95% confidence interval 1.3 to 13.0); P<0.02) of progressing to clinical albuminuria independently of treatment allocation (fig 4). Baseline glycated haemoglobin values did not influence the likelihood of progression and there was no correlation between rates of change of albumin excretion and rates of change of glycated haemoglobin concentration.
Probability of progression to clinical albuminuria in insulin dependent diabetic patients with microalbuminuria with mean blood pressure above (thin line; n=36) and below (thick line; n=34) group mean (93.6 mm Hg), independently of treatment allocation
{kind=link}
RETINOPATHY AND ADVERSE EFFECTS
This study was not designed to investigate the effect of intensive therapy on the progression of retinopathy, and only 12 patients in the conventional therapy group and 11 in the intensive therapy group had no or mild retinopathy at baseline. Changes in retinopathy were similar in the two groups. Five patients in each group experienced severe hypoglycaemia, with a total of 17 episodes in the conventional therapy group and 11 in the intensive therapy group. An episode of diabetic ketoacidosis occurred in two patients in the conventional therapy group and three patients in the intensive therapy group.
Discussion
Intensive therapy of diabetes improved glycaemic control for up to three years but did not reduce the risk of progression to clinical albuminuria or affect the rate of change in the albumin excretion rate as compared with conventional therapy. Sustained improvement of glycaemic control in the group given intensive therapy was difficult to maintain after three years despite continued high resource input, possibly because of the reduced sensitivity to insulin in patients with microalbuminuria.15
The likelihood of progression to clinical albuminuria was significantly and positively associated with the study average arterial pressure but not with the glycated haemoglobin concentration. The fall in blood pressure during the study in the conventional therapy group might therefore have confounded the outcome, but the difference in blood pressure changes between the treatment groups was not significant and adjustment for blood pressure differences did not alter the results. In the whole group the cumulative incidence of clinical albuminuria during the observation period was 21%, which accords with the findings of other studies in insulin dependent diabetic patients with microalbuminuria.16 17
Our findings contradict reports that improved glycaemic control reduces the risk of clinical albuminuria in insulin dependent diabetes mellitus complicated by microalbuminuria. The magnitude and duration of glycaemic separation between the two treatment groups were similar to those in other studies7 18 19 and should have allowed us to detect a difference in treatment effect. We cannot exclude entirely, however, the possibility that longer periods of improved control may be required to affect outcome.4 With one exception,7 all studies so far reporting a beneficial effect of intensive therapy on the progression to clinical albuminuria have included predominantly insulin dependent diabetic patients with a normal albumin excretion rate.4 18 20 These trials must therefore be considered as primary prevention studies.
Only one secondary prevention study comparable to ours included exclusively insulin dependent diabetic patients with microalbuminuria and showed no progression at all to clinical albuminuria in the group treated with insulin infusion pumps; the study also recorded a surprisingly large number of events (five out of 18) in the conventionally treated group.7 That study used a lower albumin excretion rate (20 µg/min) to define microalbuminuria, included only 18 patients in each group, and followed patients up for an average of two years, after which randomisation was broken.16 Our study was twice the size but still had a comparatively high chance of missing an effect.
The diabetes control and complications trial comprised 73 insulin dependent diabetic patients who had microalbuminuria (defined as an albumin excretion rate of 28-207.9 µg/min--a value comparable to ours) at entry. Thirty eight patients were assigned to intensive therapy and 35 to conventional therapy. Recent subanalysis showed no difference in the rate of progression to clinical albuminuria, which occurred in eight patients in each group.21
These two studies together had sufficient power to detect a reduction in the risk of progression to clinical albuminuria of 33% or greater. A smaller treatment effect cannot be excluded. The findings suggest that intensive treatment in insulin dependent diabetes complicated by microalbuminuria is likely to have a limited impact on the secondary prevention of clinical albuminuria. This should be contrasted with the 56% risk reduction achieved by intensifying treatment in insulin dependent diabetic patients with normoalbuminuria.4
The main determinant of progression in this group of insulin dependent diabetic patients with microalbuminuria seemed to be the arterial pressure rather than the blood glucose concentration. This observation has been reported by others.7 The importance of blood pressure in the progression of microalbuminuria is supported by the efficacy of antihypertensive treatment (in particular, with angiotensin converting enzyme inhibitors) in reducing the risk of clinical albuminuria.17 Thus, though blood glucose control contributes to the initiation of the renal injury--as suggested by the efficacy of primary prevention studies--once microalbuminuria has developed with the establishment of intraglomerular hypertension22 and definite renal histological lesions23 the process of progressive renal disease becomes largely independent of glucose.
In conclusion the case for intensive therapy of insulin dependent diabetes complicated by microalbuminuria rests with the observation that the clinical course of other complications such as early retinopathy and neuropathy (which are more prevalent)24 may be improved.4 25 To obtain a measurable effect on the progression of nephropathy other therapeutic strategies, such as reduction of blood pressure and angiotensin converting enzyme inhibition, must be considered as potentially preferable.
Members of the Microalbuminuria Collaborative Study Group were Colin F Close, Andrea Collins, Walter Gregory, Caron Hill, R J Jarrett, Sharon L Jones, Harry Keen, Graham S Scott, GianCarlo Viberti, Hita Vora, and Jeannie Yip, United Medical and Dental Schools of Guy's and St Thomas's Hospitals; Ana Grenfell, Alistair Mackie, Michael J Sampson, and Peter J Watkins, King's College Hospital, London; Carol Fishwick, Wendy Gatling, Ronald D Hill, and Mary Thomson, Poole General Hospital, Dorset; Sally M Marshall, University of Newcastle upon Tyne; and Philip Coates, David R Owens, John R Peters, Jiten Vora, and Susan Warren, University Hospital of Wales, Cardiff. The drafting group was G C Viberti, R J Jarrett, S L Jones, H Vora, and W Gregory.
Acknowledgments
We thank Dr N Essex, Mayday University Hospital, Croydon; Dr G Jackson, Lewisham Hospital,London; Dr C Lowy and Professor P Sonksen, St Thomas's Hospital, London; Dr P Marsden, Greenwich District Hospital, London; Professor J S Yudkin, Whittington Hospital, London; and Drs P Stephensonand J Chapman, Queen Elizabeth Hospital, Gateshead, for allowing us to study their patients; the patients for their cooperation; and Mrs B Crowe for preparing the manuscript.
Footnotes
-
Funding The Department of Health, the Juvenile Diabetes Foundation, the British Diabetic Association, and the Special Trustees of Guy's Hospital.
-
Conflict of interest None.