Re-evaluating cost effectiveness of universal meningitis vaccination (Bexsero) in England: modelling study
BMJ 2014; 349 doi: https://doi.org/10.1136/bmj.g5725 (Published 09 October 2014) Cite this as: BMJ 2014;349:g5725
- Hannah Christensen, research associate1,
- Caroline L Trotter, senior lecturer2,
- Matthew Hickman, professor of public health and epidemiology1,
- W John Edmunds, professor of infectious disease modelling3
- 1School of Social and Community Medicine, University of Bristol, Bristol BS8 2PS, UK
- 2Disease Dynamics Unit, Department of Veterinary Medicine, University of Cambridge, Cambridge CB3 0ES, UK
- 3London School of Hygiene and Tropical Medicine, London WC1E 7HT, UK
- Correspondence to: H Christensen hannah.christensen{at}bristol.ac.uk
- Accepted 22 August 2014
Abstract
Objective To use mathematical and economic models to predict the epidemiological and economic impact of vaccination with Bexsero, designed to protect against group B meningococcal disease, to help inform vaccine policy in the United Kingdom.
Design Modelling study.
Setting England.
Population People aged 0-99.
Interventions Incremental impact of introductory vaccine strategies simulated with a transmission dynamic model of meningococcal infection and vaccination including potential herd effects. Model parameters included recent evidence on the vaccine characteristics, disease burden, costs of care, litigation costs, and loss of quality of life from disease, including impacts on family and network members. The health impact of vaccination was assessed through cases averted and quality adjusted life years (QALYs) gained.
Main outcome measures Cases averted and cost per QALY gained through vaccination; programmes were deemed cost effective against a willingness to pay of £20 000 (€25 420, $32 677) per QALY gained from an NHS and personal and social services perspective.
Results In the short term, case reduction is greatest with routine infant immunisation (26.3% of cases averted in the first five years). This strategy could be cost effective at £3 (€3.8, $4.9) a vaccine dose, given several favourable assumptions and the use of a quality of life adjustment factor. If the vaccine can disrupt meningococcal transmission more cases are prevented in the long term with an infant and adolescent combined programme (51.8% after 30 years), which could be cost effective at £4 a vaccine dose. Assuming the vaccine reduces acquisition by 30%, adolescent vaccination alone is the most favourable strategy economically, but takes more than 20 years to substantially reduce the number of cases.
Conclusions Routine infant vaccination is the most effective short term strategy and could be cost effective with a low vaccine price. Critically, if the vaccine reduces carriage acquisition in teenagers, the combination of infant and adolescent vaccination could result in substantial long term reductions in cases and be cost effective with competitive vaccine pricing.
Introduction
Invasive meningococcal disease is a serious bacterial infection mainly affecting young children. The disease progresses rapidly, has a fatality rate of 5-10%,1 and a considerable proportion of survivors have long term disabling sequelae such as deafness, neurological impairments, and amputation.2 Conjugate vaccines have been successfully used to protect against disease caused by meningococci with ACWY capsular polysaccharides.3 Until recently, however, there has not been a vaccine providing broad protection against the diverse group B strains. In 2011, meningococcal group B was responsible for 82% of the 926 laboratory confirmed cases of meningococcal disease in England and Wales.4 There are natural fluctuations in the incidence of the disease over time and by location, the reasons for which are generally poorly understood, so there is uncertainty over how the incidence of disease will develop in the future and whether the current comparatively low incidence in the United Kingdom will persist, decline further, or increase.
In January 2013, Bexsero, a five component vaccine developed by Novartis to protect against group B meningococcal disease, was licensed in Europe, raising the prospect of effective control of virtually all meningococcal disease through vaccination. In July 2013, however, the Joint Committee on Vaccination and Immunisation, the independent committee advising the UK Government on vaccine policy, released an interim statement advising against the introduction of routine infant or adolescent immunisation.5 The announcement led to swift responses from charities, clinicians, academics, and politicians challenging the statement and calling for vaccine introduction.6 7 In particular the committee’s conclusion that “. . . on the basis of the available evidence, routine infant or toddler immunisation using Bexsero is highly unlikely to be cost-effective at any vaccine price. . .” was criticised as being opaque, as previous published analyses had indicated that vaccination could be cost effective at a low vaccine price.8
We assessed the epidemiological and economic impact of Bexsero vaccination in England, substantially revising a previously published mathematical model8 to incorporate new evidence and deal with the concerns raised by stakeholders as part of the consultation responses to the interim statement from the Joint Committee on Vaccination and Immunisation including: the representation of disease burden in the models, costs of treatment and care, losses of quality of life in affected patients and those close to them, litigation costs, and the appropriate choice of discount rate for public health interventions.
Methods
Model
There is evidence to suggest Bexsero can disrupt meningococcal carriage9 so we used a transmission dynamic model to capture both the direct and indirect effects of vaccination in England. We used a susceptible-infected-susceptible (SIS) model to represent the transmission of meningococcal carriage (fig 1⇓). This model is described fully elsewhere8 and briefly here. The model is structured into 100 age classes (0-99 years). Individuals are born susceptible (S), might become carriers of a meningococcal strain that is vaccine preventable (M) or non-vaccine preventable (N), and after a period of time clear carriage and recover (r) to return to the susceptible state.
Age specific forces of infection were assumed to be constant over time for meningococcal strains that are non-vaccine preventable. The force of infection for strains that are vaccine preventable varies over time according to the number of carriers of vaccine preventable strains in the population and age specific contact rates. Cases are generated by applying a case:carrier ratio to the number of new carriage acquisitions by using previously specified functions8 (fitted values are presented in table 1⇓). Age specific rates of disease incidence were based on all meningococcal capsular groups.
Parameters for risk of developing invasive disease after person has become infected for baseline dynamic model, estimated with data on disease incidence from 2005-06 to 2011-12, and duration of carriage of six months in study of re-evaluating cost effectiveness of vaccination (Bexsero) against meningococcal disease
We considered all serogroups in our model because, though Bexsero was designed to protect against meningococcal group B, the protein antigens in the vaccine are also present in non-group B strains and thus it can be expected to offer some protection against non-group B strains.
The age specific population was based on a 2011 birth cohort experiencing current rates of natural mortality. When vaccination is introduced, a proportion of individuals move into vaccinated compartments dependent on the age specific uptake rate (ui) (fig1⇓). Vaccinated individuals were assumed to acquire immunity after their second dose of vaccine. Vaccinated individuals with immunity (compartments VNIi, VSIi, and VMIi) could have a degree of protection against carriage acquisition as well as disease. Immunity can wane over time, in which case individuals then have the same risks of infection as unvaccinated individuals (compartments VNi, VSi, and VMi). Vaccination compartments were further stratified into routine infant, routine adolescent, or catch up programmes to allow for different durations of protection from vaccination between the different elements of the vaccine programme, as was seen after the meningococcal group C conjugate vaccine campaign.10
The model was parameterised by using carriage estimates from a recent systematic review11 and disease data for England by using an assortative population mixing pattern, found to perform well in modelling of meningococcal group C vaccination in the UK.12 After meningococcal disease, individuals can survive without sequelae, survive with sequelae (with a reduced quality of life), or die. We also included non-meningococcal deaths and adjusted natural mortality rates to remove deaths from meningococcal disease as these are modelled separately. We ran models for a 100 year period with all parameters respecting this time horizon to capture the costs and benefits of vaccination over people’s lifetimes. For routine programmes with vaccination each year this means some cohorts have incomplete follow-up in the model, although the effects of this are mostly mitigated through discounting future costs and benefits.
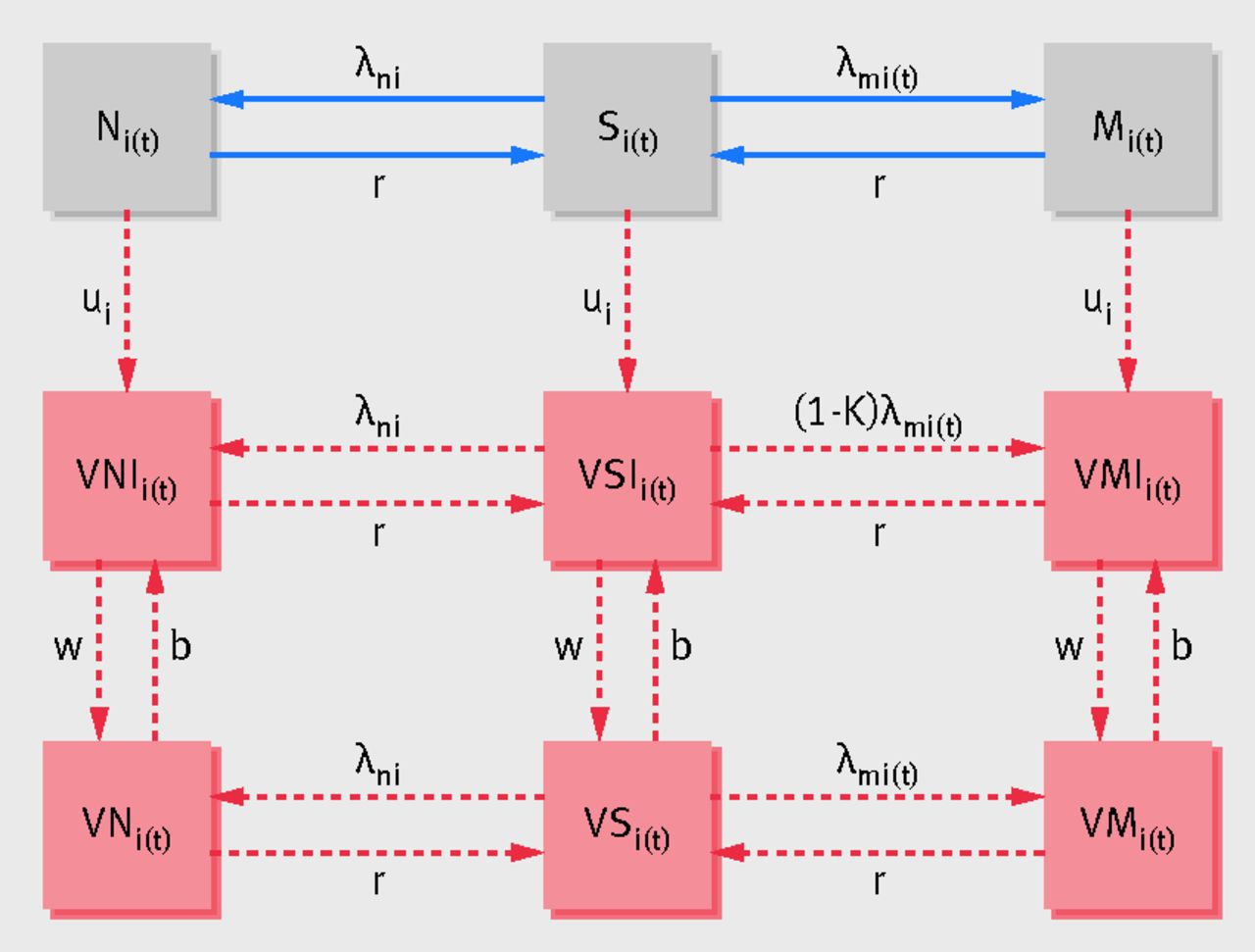
Fig 1 Dynamic model structure. “No vaccination” model consists of grey boxes and blue arrows; “with vaccination” model includes red shaded boxes and red dashed arrows in addition. Once individuals acquire carriage they have chance of developing disease, resulting in either survival without sequelae, survival with sequelae, or death. S= susceptible non-vaccinated; M=infected carrier of vaccine preventable meningococcal strain; N=infected carrier of non-vaccine preventable meningococcal strain; VSI=susceptible vaccinated and immune; VMI=infected carrier of vaccine preventable meningococcal strain, vaccinated and immune; VNI=infected carrier of non-vaccine preventable meningococcal strain, vaccinated and immune; VS=susceptible vaccinated not immune; VM=infected carrier of vaccine preventable meningococcal strain, vaccinated not immune; VN=infected carrier of non-vaccine preventable meningococcal strain, vaccinated not immune; λm=force of infection for vaccine preventable meningococcal strains; λn=force of infection for non-vaccine preventable meningococcal strains; κ=vaccine efficacy against carriage acquisition; u=vaccine uptake; w=waning vaccine protection; b=vaccination booster; i=age; t=time. Reprinted from Christensen et al8with permission from Elsevier
{kind=link}
Parameter values
Full details of the model parameters are in the appendix. The Joint Committee on Vaccination and Immunisation considered several iterations of analyses of the impact and cost effectiveness of different vaccination strategies with Bexsero. Table 2 shows changes in the sources of data used previously and the inclusion of certain types of data for comparison.⇓
Changes in data sources included in modelling assessment of impact and cost effectiveness of vaccination (Bexsero) against meningococcal disease according to timing of consideration by Joint Committee on Vaccination and Immunisation
Recent surveillance data from laboratory confirmations and hospital episode statistics (HES) indicate that the numbers of cases of meningococcal disease continues to decline, thus the time period chosen for calculations is important. Data from the Notifications of Infectious Disease provides the longest time trend for meningococcal cases in England and Wales, though interpreting these data is complicated by the fact that reporting has changed over time (fig 2⇓). In addition to the natural fluctuation in case numbers, large increases were associated with the two world wars, and the introduction of the meningococcal group C conjugate vaccine in 1999 resulted in a substantial decrease in cases. We used an average incidence over a longer time period (2005-06 to 2011-12) than used previously8 to account for long term trends and used hospital episode statistics data as not all cases are laboratory confirmed.

Fig 2 Number of cases of meningococcal disease over time in England and Wales. Principal data from Notifications of Infectious Disease (NOIDS) for England and Wales,38 39 with sections indicating diseases reported during different time periods. Reference lines for England estimates based on hospital episode statistics data
{kind=link}
We included losses of quality of life during the acute disease episode, deriving estimates from a recent Public Health England study using EQ-5DY in children up to a year after the illness (Iain Kennedy, personal communication). Long term reductions in quality of life for survivors with sequelae were estimated by using data from the MOSAIC study (appendix), a case-control study of children surviving meningococcal group B disease.2 The proportion of survivors with sequelae and the long term cost (health and personal and social services) were estimated from the same study. Some cases were assumed to result in claims against the NHS, attracting legal costs and damages not related to quality of life (damages related to quality of life were not included because loss of quality of life is explicitly modelled as utility loss, thus costs to compensate for such loss are not included to avoid double counting). Litigation costs have not historically been considered in models that assess vaccine impact in the UK but do represent costs to the NHS and thus are included here based on data from the NHS Litigation Authority. We assumed the total cost was split into 20 equal annual payments and allowed for a delay in the case arising and the first payout to allow for the legal process.
The Joint Committee on Vaccination and Immunisation code of practice states adjustment factors should be applied to modelled benefits or costs when there is good reason to believe that these are underestimated or overestimated and that the incremental cost effectiveness ratio should then be judged against a £20 000 threshold per quality adjusted life year (QALY).13 This is analogous to the National Institute for Health and Care Excellence approach of allowing technologies, given certain situations, to be recommended at thresholds above £20 000. The use of an adjustment factor was first raised by the Joint Committee on Vaccination and Immunisation in relation to Bexsero and meningococcal disease in April 2013.14 Because of concerns over whether the EQ-5D could fully capture long term losses of utility in survivors of meningococcal disease or losses in children, considerations of the differential societal value of equal QALY measures of severe and relatively mild disease, and the innovative nature of the Bexsero vaccine, in October 2013 the Joint Committee on Vaccination and Immunisation specified a QALY adjustment factor (QAF) of three for use in the models.15 Currently unpublished work from Al-Janabi and colleagues has shown losses of quality of life in family of survivors and network members as well as survivors themselves.16 In a UK wide prospective cross sectional study of 1600 individuals close to someone who had survived meningitis, they estimated the impact of sequelae on family members’ quality of life. Aggregating quality of life losses in the family network, they estimated that the losses of quality of life to the family network could be around 48% of the size of quality of losses to the survivor, in families in which the person with disease had sequelae. Based on this evidence, in modelled scenario analyses we assumed the loss of quality of life to the family and network to be proportional (48%) to that experienced by the patient and is therefore affected by the choice of quality of life adjustment factor. The study by Al-Janabi and colleagues did not measure the impact of death on family members’ quality of life, therefore a modification was made to account for QALYs being lost in bereaved family members rather than through sequelae (using evidence of the impact of bereavement on parents’ quality of life17 and comparing the loss of quality of life experienced by survivors with sequelae in the study with the loss of quality of life from death). In this case the additional loss of quality of life experienced by the bereaved family and network members was assumed to be equivalent to 9% of the QALYs lost by the death of the person with meningococcal disease.
Vaccine strategies and characteristics
We considered several vaccine strategies (table 3⇓), targeting age groups in which incidence is high (infants) and transmission is thought to be greatest (adolescents). We assumed 88% vaccine strain coverage based on a study that used a serum bactericidal antibody assay (which seems more sensitive than the meningococcal antigen typing system (MATS) test).18 Vaccinated individuals were assumed to have 95% protection against disease based on immunogenicity studies19 20 and 30% protection against carriage acquisition based on a recent trial.9 The duration of vaccine protection was based on data from clinical trials of Bexsero and estimates from other meningococcal vaccines in use, such as the meningococcal group C conjugate vaccine. We included the costs of treating medically attended adverse reactions but not related losses of quality of life as the adverse reactions were assumed to be of short duration and without lifelong effects. Because of concerns around fever rates when Bexsero is given concomitantly with other vaccines, we included separate rates and costs for medically attended mild fever (age stratified), which were assume to require a GP consultation, and febrile convulsions requiring a hospital admission. We also included mild non-fever reactions requiring a GP visit and anaphylaxis requiring a hospital stay.
Vaccination strategies modelled with base case vaccination parameters in re-assessment of cost effectiveness of vaccination (Bexsero) against meningococcal disease
Vaccine trials measured antibody responses one month after receipt of the vaccine so protection is assumed to start one month after the second dose. In the reduced infant schedule specified by the Joint Committee of Vaccination and Immunisation (2, 4, and 12 months), protection was assumed to start five days after the second dose; though this schedule is “off indication,” studies have shown good antibody responses after two vaccine doses21 and observations from other vaccines have shown notable increases in antibody titres five to seven days after vaccination. While Bexsero was designed to protect against capsular group B meningococci, the protein antigens in the vaccine are also present in non-group B strains. Given this, we investigated the effect of removing the infant (3 month) meningococcal group C conjugate vaccine dose while delivering infant vaccination with Bexsero according to the licensed indication (three priming doses and a booster). We assumed this would not affect the number of cases of group C meningitis observed because a teenage meningococcal group C conjugate booster has recently been introduced, which is anticipated to maintain herd protection, and the use of Bexsero in infancy can be expected to provide a level of direct protection against group C cases in this age group (thus the net change in this scenario is to reduce the cost of meningococcal vaccination only). The price paid by the UK government for vaccines is confidential, therefore we assumed a meningococcal group C vaccine cost of £7.50 (€9.53, $12.25), the current list price for Meningitec.22
Cost effectiveness analyses
Our primary outcomes were cases and deaths averted and QALYs gained under vaccination, compared with the current situation in which cases are treated as they arise. Costs were measured in pounds at 2011 prices, with costs from previous years inflated with the Hospital and Community Health Services pay and price index. Costs and benefits were assumed to occur at the start of the year, with future costs and benefits discounted at 3.5%23 (base case) or 1.5%.24 Analyses were undertaken from the NHS and personal and social services perspective and strategies were considered cost effective if the discounted cost per QALY gained was <£20 000.13
Scenario analyses
We ran scenarios assuming no herd effects, higher and lower vaccine strain coverage, lower disease incidence, with and without litigation costs and family and network losses of quality of life, and excluding the quality of life adjustment factor.
Results
The model estimates 1447 cases of meningococcal disease (all capsular groups) and 59 deaths occur annually in the absence of vaccination against group B meningococcal disease. We predict that in the first five years of a 2, 3, 4, and 12 month infant programme, 26.3% of cases would be averted (fig 3⇓); this relatively low percentage, despite the high vaccine uptake, is driven by the short duration of vaccine protection and incomplete vaccine strain coverage. Projections for cases averted under the 2, 4, and 12 months strategy are only 0.3% lower than for the 2, 3, 4, and 12 months schedule because the level of protection is assumed to be almost identical. In the short term maximal case reduction is achieved through routine infant vaccination with one-off catch up in children aged 1-4 years.

Fig 3 Effect on annual disease cases of alternate vaccination strategies. VEC=vaccine efficacy against carriage, SC=strain coverage, CU=one-off catch up vaccination. Switching strategy refers to routine vaccination infant at 2, 3, 4, and 12 months and adolescent at 13 years (two doses), switching after 10 years to routine infant at 2, 4, and 12 months and adolescent at 13 years (two doses)
{kind=link}
Long term maximal reduction is achieved by combining routine infant (2, 3, 4, and 12 months) and adolescent (13 years) vaccination, reducing annual cases by 48.8% in 10 years and 59.7% in 20 years. Adolescent vaccination without an infant programme, however, has little short term impact (3.4% case reduction over five years) because the highest incidence of disease is in young children and it takes considerable time for herd effects to protect infants (fig 3⇑ and fig 4⇓). While individuals would require six doses for a combined infant and adolescent programme, a phased reduction could be possible once herd effects are established, removing the dose at 3 months 10 years into the programme as part of a switching strategy; this could prevent 46.2% of cases over 20 years.

Fig 4 Cases averted through routine adolescent vaccination by age group at selected time points since start of vaccination, with different assumptions on vaccine efficacy against carriage acquisition (VEC)
{kind=link}
In the principal analyses none of the programmes were cost effective at the Bexsero list price (£75 a dose, table 4⇓). With a reduction in vaccine price, however, all strategies could be cost effective, albeit in some cases at low prices (≤£3 a dose for routine infant vaccination). Use of a reduced schedule in infants or removal of the infant meningococcal group C vaccine results in a considerable reduction in programme costs, thus these strategies could be cost effective at higher vaccine prices (£6-7 a dose). In formal incremental analyses, adolescent vaccination with catch up was relatively the most cost effective strategy; all strategies without adolescent vaccination were dominated. Though 1.5% discounting for costs and benefits increased the threshold vaccine prices, they all remained well below the list price.
Results from dynamic model of cost effectiveness of vaccination (Bexsero) against meningococcal disease. Comparison of vaccination strategies (vaccination v no vaccination) assuming 30% vaccine efficacy against carriage acquisition
The results are highly sensitive to vaccine profile assumptions (table 5⇓). If we assume no herd effects, maximal case reduction is achieved by targeting infants in whom disease incidence is high; even without herd effects 24% of cases are averted over five years (2, 3, 4, and 12 month programme). This strategy could be cost effective at £1 a dose. With only direct protection, adolescent vaccination averts few cases because of the low incidence in this age group (4.2% over 20 years) and is not cost effective at any vaccine price. Scenarios that assume vaccine efficacy against carriage of 10% or 20% illustrate that herd effects are critical for the impact and cost effectiveness of routine adolescent vaccination, but because of the assumed low carriage prevalence in infants the assumed vaccine impact on carriage is less important in the consideration of routine infant vaccination alone (table 6⇓). The predicted vaccine strain coverage by the meningococcal antigen typing system test varies by country because of variations in the circulating strains and can be used as a proxy for changes in strain coverage over time within a country. If the lowest known strain coverage (66%, Canada) is combined with the assumption of no herd effects (fig 5⇓), the only cost effective strategies are those in infants with removal of a dose of meningococcal vaccine with a vaccine price of £1-2 a dose. The assumed duration of protection is also particularly important for adolescent strategies; if the vaccine protected individuals for an average of three rather than 10 years, vaccination would not be cost effective with 3.5% discounting, even with herd effects (table 6⇓).

Fig 5 Effect on annual cases of disease of varying assumptions for vaccine strain coverage and efficacy against carriage acquisition for routine infant or adolescent vaccination. VEC=vaccine efficacy against carriage, SC=strain coverage
{kind=link}
Results from dynamic model of cost effectiveness of vaccination (Bexsero) against meningococcal disease. Comparison of vaccination strategies (vaccination v no vaccination) assuming 0% vaccine efficacy against carriage acquisition
Selected scenarios from dynamic model of cost effectiveness of vaccination (Bexsero) against meningococcal disease (vaccination v no vaccination)
In scenario analyses we combined several vaccine favourable and conservative parameters (table 7⇓). These are extreme scenarios because it is unlikely that all positive or negative assumptions will coincide, however they frame the range of possible outcomes. Under “vaccine conservative” assumptions (lower disease incidence, 66% strain coverage, no herd effects or litigation costs) the percentage of cases averted is 40% lower than the base case, and none of the strategies is cost effective at any vaccine price. With “favourable” assumptions (91% strain coverage, 60% vaccine efficacy against carriage, including litigation costs and losses of quality of life in family and network members, with 1.5% discounting) all strategies are cost effective if the vaccine is competitively priced (£14 a dose for 2, 3, 4, and 12 months vaccination, £20 a dose for routine infant and adolescent vaccination, and £63 a dose for adolescent vaccination alone).
Results from dynamic model of cost effectiveness of vaccination (Bexsero) against meningococcal disease. Comparison of vaccination strategies (vaccination v no vaccination) assuming vaccine favourable or conservative parameters
The valuation of the impact of disease on the person directly affected as well as their family and network members has a large influence on the cost effectiveness of vaccination. Under the infant programme, inclusion of losses of quality of life in the family and network members of those affected by meningococcal disease doubles the threshold vaccine price that would be considered cost effective (table 6⇑). Removal of the quality of life adjustment factor from the analyses considerably reduces the estimated QALYs gained through vaccination, with the infant programme not reaching the cost effective threshold at any vaccine price with 3.5% discounting.
Discussion
Principal findings
Our findings indicate that infant immunisation against meningitis (at 2, 3, 4, and 12 months) maximises case reduction in the short term, preventing 26.3% of cases in the first five years of the programme, and could be cost effective with the vaccine priced at £3 a dose assuming 88% vaccine strain coverage, 30% efficacy against carriage acquisition, and 95% efficacy against disease, disease incidence based on a long term average, and with the inclusion of a quality of life adjustment factor. If similar levels of protection could be achieved with removal of the infant meningococcal group C conjugate vaccine or by using a 2, 4, and 12 months schedule this would be more economically favourable and could be cost effective at a cost of £6-7 a dose, or up to £22 a dose if several further vaccine favourable assumptions were combined. Routine adolescent vaccination is the superior strategy economically but depends critically on the vaccine disrupting meningococcal transmission and takes many years to have any real impact on disease if it is used without an infant programme. Combined infant and adolescent strategies achieve the greatest impact (29.1% reduction over five years, 37.0% over 10 years) and are cost effective at a cost of £4-6 a dose. Modification of the discount rate to 1.5% for costs and benefits instead of 3.5% improves the cost effectiveness of vaccination.
Strengths and limitations
We have incorporated new evidence and covered key concerns of stakeholders and critics of the original interim statement from the Joint Committee on Vaccination and Immunisation. While NICE guidance states that health outcomes should be included for patients and carers,23 24 in practice this is rarely done. We have shown in scenario analyses that their inclusion can considerably improve the cost effectiveness of vaccination
Ours is not the first modelling study to consider losses of quality of life in people other than those directly affected by the disease.25 Given that it can be argued that there are implications for family and network members with any disease, and that the addition of “network quality of life losses” can alter the vaccine price that is considered cost effective, it is important that methods supporting policy decisions are consistent. We used a transmission dynamic model to appropriately capture both the direct and indirect effects of vaccination and show that the impact of Bexsero on carriage is critical to the impact on public health and the cost effectiveness of vaccination, particularly for adolescent strategies.
Assumptions about disease incidence are also highly influential. We are currently experiencing low rates of disease, which might increase in the future, thus we used an average incidence of disease over several years and used data from hospital episode statistics, which allows for the under-ascertainment of cases through laboratory confirmations alone; this does mean, however, that the base case model assumes a much greater incidence than currently experienced, which in the short term is vaccine favourable.
Because of the potentially high rates of fever in infants when Bexsero is given concomitantly with other vaccines, options are currently being considered for the provision of prophylactic paracetamol, though we chose not to include this in our models principally because it is not clear if and how this would be provided by the NHS. Concomitant paracetamol with routine vaccinations has not previously been recommended because of evidence indicating that this could result in lower antibody responses to some antigens.26 A recent study considering prophylactic paracetamol given with routine vaccinations and Bexsero, however, resulted in reduced rates of fever in infants with no apparent clinically relevant decreases in immune responses to any of the vaccines given.27
We recognise that mathematical models are a simplification of the real world setting. We assumed that the life expectancy for survivors of meningococcal disease is the same as those who have not experienced the disease. There is some evidence suggesting this is not the case,28 though the differences seem small. While this would lead to underestimation of QALY gains through vaccination, we believe this is outweighed by the fact the model assumes a perfect state of health for individuals not affected by disease, though this declines with age.29 Our model captures the long term costs of care for those with sequelae in a simple form, assuming a constant cost over the person’s life when in fact support needs might change. Because of the availability of data, we took a similar approach for the family and network impact of disease. We included costs, but not losses of quality of life, for vaccine adverse reactions as is standard practice. While these reactions are transient, inclusion of impacts on quality of life would result in vaccination seeming less economically favourable. Our models do not include strain replacement or the possible negative effects of reducing bacterial carriage, thus might be optimistic.
Comparison with other studies
Several European countries have considered, but not recommended, universal vaccination. In France,30 the Netherlands,31 and Ontario, Canada,32 economic models indicated that vaccination was unlikely to be cost effective; in Spain the vaccine was not recommended on epidemiological grounds.33 Thus far the vaccine has been used only in the private market in Europe and in response to outbreaks in the United States, although currently unlicensed there. A modelling study by the manufacturer considering the epidemiological impact of Bexsero also found that maximal case reduction was achieved through routine infant vaccination in the short term and adolescent vaccination in the long term, assuming a high vaccine efficacy against carriage (67%).34 A study in Normandy that used a meningococcal group B outer membrane vesicle based vaccine (a component of Bexsero) found high levels of protection (85% carriage reduction in unadjusted analyses), but few carriers were observed overall.35 Results from a clinical trial of Bexsero on carriage suggest that the individual impact is considerably lower.
Implications for policy makers
While a probabilistic model would allow the parameter uncertainty to be fully captured, the substantial uncertainty surrounding vaccine protection is unlikely to be resolved without its use in a population setting. Given this, policy makers must make judgments about which assumptions are more likely, whether cost effectiveness is key, and, if not, under what circumstances should vaccination be implemented. We undertook substantial scenario analyses, including combinations of favourable and conservative vaccine assumptions, to provide estimates of the upper and lower bounds for impact and cost effectiveness. Models can be valuable tools to gain a greater understanding of the potential impact of an intervention, but there is inherent uncertainty associated with such modelling and value judgments need to be made.36 There is considerable demand for the meningococcal vaccine, both from the public and from clinicians, driven by the severity of the disease and the fact that children are those at greatest risk. Proponents argue that preventive interventions, particularly in children, should be given greater weight and that society places greater value on averting rare cases of severe disease rather than frequent instances of mild disease.37 Models can inform decision makers of the impact of such alternative preferences.
Our findings have informed the Joint Committee on Vaccination and Immunisation statement on the use of Bexsero in the UK, which can recommended a vaccine only if it is deemed cost effective.13 The consideration of Bexsero is the first time the committee has used the guidance from the Working Group on Uncertainty in Vaccine Evaluation and Procurement to assess the cost effectiveness of vaccination, including the provision for quality of life and cost adjustment factors. This method represents a change in the process of vaccine assessment but is analogous to NICE’s method of technology assessment, in which technologies might be approved, in special circumstances, even if the incremental cost effectiveness ratio is above £20 000. It will be important that the Joint Committee on Vaccination and Immunisation is explicit about the reasons and justification for the value of the adjustment factors to ensure consistency across vaccine decisions.
Conclusions
Our results suggest that routine infant vaccination could be cost effective in England under favourable assumptions if the vaccine could be procured at <20% of the list price. This is the most favourable option because it targets those most at risk of disease, and the impact of uncertainty over carriage disruption is limited because carriage prevalence is low in young children.11 The impact of a routine adolescent programme rests on how much the vaccine disrupts carriage, and further research is needed to answer this question. Surveillance after implementation will be crucial to determining the true effectiveness of the vaccine.
What is already known on this topic
The first broadly protective vaccine against meningococcal group B disease (Bexsero) was licensed in Europe in January 2013
In July the Joint Committee on Vaccination and Immunisation advised against the introduction of this vaccine in the UK on grounds of cost effectiveness; no other country has yet recommended vaccination
The UK interim statement was challenged by charities, clinicians, academics, and politicians, who called for introduction of the vaccine, particularly as previous published analyses had indicated that it could be cost effective
What this study adds
Model estimates incorporating new evidence and a quality of life adjustment factor and covering key concerns of critics of the Joint Committee on Vaccination and Immunisation interim statement indicate that infant immunisation maximises case reduction in the short term (preventing 26.3% of cases in the first five years) and could be cost effective in England under favourable assumptions with a low vaccine price (range £3-22)
These results have been used to inform the committee’s final statement on the use of Bexsero in the UK, which recommended routine infant immunisation at 2, 4, and 12 months of age, subject to a cost effective vaccine price
Notes
Cite this as: BMJ 2014;349:g5725
Footnotes
We thank the following individuals for providing data and assistance: Mary Ramsay, Shamez Ladhani, and Iain Kennedy (Public Health England); Hareth Al-Janabi (University of Birmingham); Charlotte Chamberlain and Laura Clark (University of Bristol); Julie Mills (Office for National Statistics); and Guy Walker (Department of Health). The hospital episode statistics data were made available by the NHS Health and Social Care Information Centre. Copyright © 2013. Re-used with the permission of the Health and Social Care Information Centre. All rights reserved.
Contributors: All authors were involved in the conception and design of the research. HC, CLT, and JE developed the models; HC analysed and all authors interpreted the results. HC wrote the first draft of the manuscript; all authors drafted the final version of the manuscript. All authors had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. HC and WJE are guarantors.
Funding: This work was supported by the Department of Health and the National Institute for Health Research (NIHR) (RDA/03/07/014 and PDF-2012-05-245 to HC, PDA/02/06/088 to CT). This work is produced by the authors under the terms of these research training fellowships issued by the NIHR. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. MH is a member of the NIHR School of Public Health Research; HC and MH are members of the NIHR Health Protection Research Unit Evaluation of Interventions. The sponsors of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Competing interests: All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that HC, MH, and WJE have support from the Department of Health for the submitted work.
Ethical approval: Not required.
Transparency declaration: The lead author affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Data sharing: Details of the model data inputs and other assumptions are provided in the methods and supporting parameters table. Researchers interested in further details of the model can contact the corresponding author.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.