Mortality in British military participants in human experimental research into chemical warfare agents at Porton Down: cohort study
BMJ 2009; 338 doi: https://doi.org/10.1136/bmj.b613 (Published 25 March 2009) Cite this as: BMJ 2009;338:b613
- K M Venables, reader in occupational medicine1,
- C Brooks, data manager 1,
- L Linsell, medical statistician1,
- T J Keegan, research fellow1,
- T Langdon, assistant data manager1,
- T Fletcher, senior lecturer in environmental epidemiology2,
- M J Nieuwenhuijsen, research professor in environmental epidemiology3, visiting professor4,
- N E S Maconochie, senior lecturer in epidemiology and medical statistics5,
- P Doyle, professor of epidemiology5,
- V Beral, professor and director 6,
- L M Carpenter, reader in statistical epidemiology1
- 1Department of Public Health, University of Oxford, Oxford OX3 7LF
- 2Department of Public Health and Policy, London School of Hygiene and Tropical Medicine, London
- 3Centre for Research in Environmental Epidemiology, IMIM and CIBERESP, 08003 Barcelona, Spain
- 4Division of Epidemiology, Public Health and Primary Care, Imperial College, London
- 5Department of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London
- 6Cancer Epidemiology Unit, University of Oxford, Oxford
- Correspondence to: K M Venables kate.venables{at}dphpc.ox.ac.uk; L M Carpenter lucy.carpenter{at}dphpc.ox.ac.uk
- Accepted 5 December 2008
Abstract
Objective To investigate any long term effects on mortality in participants in experimental research related to chemical warfare agents from 1941 to 1989.
Design Historical cohort study.
Data sources Archive of UK government research facility at Porton Down, UK military personnel records, and national death and cancer records.
Participants 18 276 male members of the UK armed forces who had spent one or more short periods (median 4 days between first and last test) at Porton Down and a comparison group of 17 600 non-Porton Down veterans followed to 31 December 2004.
Main outcome measures Mortality rate ratio of Porton Down compared with non-Porton Down veterans and standardised mortality ratio of each veteran group compared with the general population. Both ratios adjusted for age group and calendar period.
Results Porton Down veterans were similar to non-Porton Down veterans in year of enlistment (median 1951) but had longer military service (median 6.2 v 5.0 years). After a median follow-up of 43 years, 40% (7306) of Porton Down and 39% (6900) of non-Porton Down veterans had died. All cause mortality was slightly greater in Porton Down veterans (rate ratio 1.06, 95% confidence interval 1.03 to 1.10, P<0.001), more so for deaths outside the UK (1.26, 1.09 to 1.46). Of 12 cause specific groups examined, rate ratios in Porton Down veterans were increased for deaths attributed to infectious and parasitic (1.57, 1.07 to 2.29), genitourinary (1.46, 1.04 to 2.04), circulatory (1.07, 1.01 to 1.12), and external (non-medical) (1.17, 1.00 to 1.37) causes and decreased for deaths attributed to in situ, benign, and unspecified neoplasms (0.60, 0.37 to 0.99). There was no clear relation between type of chemical exposure and cause specific mortality. The mortality in both groups of veterans was lower than that in the general population (standardised mortality ratio 0.88, 0.85 to 0.90; 0.82, 0.80 to 0.84).
Conclusions Mortality was slightly higher in Porton Down than non-Porton Down veterans. With lack of information on other important factors, such as smoking or service overseas, it is not possible to attribute the small excess mortality to chemical exposures at Porton Down.
Introduction
After the use of chemical warfare agents in the first world war, the UK government initiated research at Porton Down to study their potential impact on military capability and the effectiveness of protective measures.1 2 3 4 5 This included a “human volunteer programme” in which, since 1916, at least 30 000 people, mainly servicemen are thought to have taken part.3 After ex-servicemen expressed concern about whether participation might have damaged their health in the long term, the UK government commissioned this epidemiological study in 2002. There have been few studies of participants in such human experimental programmes6 7 8 9 and results from mortality studies in American servicemen have been inconclusive.7 8 9 10 A recent survey of members of a UK veterans’ support group found them to report poorer quality of life than the general population.11 This is the first report of mortality and cancer morbidity12 in the cohort of British participants in the chemical tests at Porton Down.
Methods
Assembly of the Porton Down veteran cohort
Our pilot study found that service number, essential for retrieving military personnel files, was routinely recorded at Porton Down only from 1 April 1941. Our cohort comprised all members of the UK armed forces recorded as having participated in the “human volunteer programme” from 1 April 1941 to 31 December 1989. We initially identified potential cohort members using a database of 20 006 names previously abstracted by a team employed by the Ministry of Defence from documents in the historical archive at Porton Down. This was compared against the names identified during our abstraction of exposure data.
Names and service numbers were submitted to the relevant military personnel records authority: army, air force, navy, and marines. We excluded civilian staff (n=344) and members of non-UK armed forces (n=220). Personnel files were successfully retrieved for 18 441 Porton Down veterans, and identifiers necessary for data linkage were manually abstracted and entered with a standard format onto a secure computer. For army veterans, this was carried out by a team of six people employed by the University of Oxford and based at the army personnel archive. For army personnel still in active service, and for air force, navy, and marine veterans, Ministry of Defence employees trained by the research team abstracted data. The research team directed quality control procedures at all sites.
Where possible, data on service number, name, sex, date and place of birth, mother’s maiden name, NHS number, national registration identity number, national insurance number, dates of recruitment and discharge (with corresponding addresses, service numbers, and ranks), and date of death were abstracted. Names of veterans whose personnel files could not be located after identification details were checked and after a second attempt at file retrieval were submitted to the Ministry of Defence for circulation to relevant central departments. All data abstracted from personnel files were returned to the university and checked for data abstraction or entry errors. Any data discrepancies later identified were corrected, when appropriate.
Assembly of the comparison cohort
We identified a comparison group of veterans who did not visit Porton Down (“non-Porton Down veterans”). Our pilot study showed that a sample of veterans with adjacent service numbers to Porton Down veterans had similar distributions of important characteristics, such as date of birth. So, within each branch of the military, we generated a service number adjacent to (above or below) that of each Porton Down veteran and retrieved the corresponding personnel file for data abstraction and entry in the same way as for the Porton Down veterans. If a file was not found, the alternative adjacent service number was submitted and, if necessary, the process repeated. Personnel files were successfully retrieved for 18 103 non-Porton Down veterans and over 95% had service numbers immediately adjacent to the corresponding Porton Down veteran.
Follow-up
The primary source of mortality data in the UK is the National Health Service central register (NHSCR). We submitted the required identification details to the register in Southport, which traced deaths, and, when available, emigrations, for England and Wales, and managed personnel data submission for tracing to the registers in Scotland and Northern Ireland. Untraced veterans were checked against the website of the Commonwealth War Graves Commission (CWGC), a registry of deaths in Commonwealth service personnel occurring in the two world wars between 1914 and 1947 (www.cwgc.org). Names not traced by NHSCR and not found on the commission’s website were submitted to the Department for Work and Pensions (DWP) for classification as dead, alive, or vital status not known. For veterans identified by the DWP as having died, we obtained copies of death certificates, when available, from NHSCR.
Each condition on the death certificate, including the underlying cause, was coded by the Office for National Statistics according to ICD-10 (international classification of diseases, 10th revision). Death certificates were not available for deaths not registered in the UK, so cause of death was unknown.
Exposures of Porton Down veterans
To assess exposure we used contemporaneous experimental records in the Porton Down historical archive following a protocol reported elsewhere.13 14 In brief, data abstraction involved linking, when possible, each test to an individual veteran and the classification of that test as involving a chemical or not. Each chemical test was classified as involving vesicant(s), nerve agent(s), or other chemical(s). For vesicants (blistering agents) and nerve agents, detailed information relating to exposure was abstracted.14 For analyses reported here, we grouped Porton Down veterans as ever or never exposed at least once to any chemical, any vesicant, any nerve agent, or any other chemical, and to specific chemicals to which at least 1000 veterans had been exposed. “High” exposure subgroups were defined as elsewhere.14
Mortality analysis
We decided on the classifications of exposures and causes of death before we linked the exposure and outcome databases. Analyses reported relate to underlying cause of death in 18 276 male Porton Down veterans and 17 600 male non-Porton Down veterans, excluding women (134 and 127 respectively) and men with missing data (31 and 376 respectively). All analyses used STATA version 8.2 (www.stata.com). Significance was defined as P<0.05 with two sided tests.
Comparison with national mortality rates—Person years of follow-up for Porton Down veterans started from the earliest date (after 1 April 1941) they were recorded as included in a test at Porton Down; for the 973 for whom a test date was not available, we counted person years from the date of arrival at Porton Down as recorded in the Ministry of Defence database. Person years for non-Porton Down veterans started from a date derived by adding to the enlistment date the interval between the dates of the corresponding Porton Down veteran’s enlistment and first visit to Porton Down. For the 65 non-Porton Down veterans for whom we did not know date of enlistment, we counted person years from the same date as for the corresponding Porton Down veteran. Person years stopped at the earliest of date of death, loss to follow-up, or 31 December 2004. For losses to follow-up, we censored person years at the last known date alive in the UK (such as date of emigration or date of discharge from the services). We stratified person years and deaths according to 15 five year age groups (15-19, 20-24, etc, to ≥85) and by single calendar year (from 1941 to 2004). We calculated expected deaths by multiplying the person years for each five year age group and single calendar year by the corresponding national rates for England, Wales, and Scotland and estimated standardised mortality ratios from the ratio of observed to expected deaths. We obtained 95% confidence intervals and tests of significance using the normal approximation to the Poisson distribution.
Comparison of mortality between Porton Down and non-Porton Down veterans—Person years were calculated as above except that we did not censor losses to follow-up at the last known date alive in the UK. We estimated adjusted rate ratios and 95% confidence intervals and derived P values by the Mantel-Haenszel method with deaths and person years stratified according to five year age groups (as above) and five year calendar periods (1941-4, 1945-9, etc, to 2000-4).15 When the number of expected deaths in either group of veterans was less than 10, we estimated adjusted rate ratios and tested for significance by fitting exact conditional Poisson regression models to the stratified data.16 Following the approach to exposure outlined above, we compared mortality rates in specific exposure groups of Porton Down veterans with that of all non-Porton Down veterans. For groups of causes where there was either a prior hypothesis of association, or the data suggested an association, we calculated rate ratios for subgroups with “high” exposure.14
Results
Of the Porton Down veterans, 62% (11 407/18 276) had joined the army, 22% (4026) the air force, and 16% (2843) the navy, including the marines. As expected, the distribution of service at enlistment of the 17 600 non-Porton Down veterans was virtually identical (table 1)⇓. Most veterans were born in England before 1940 and joined the British armed services as teenagers during periods of conscription, either in the second world war (1939-45) or in the period of compulsory male military service (“national service”) after the war to 1960 (table 1).⇓ The median year of enlistment was 1951 for both groups. Almost all had enlisted with the rank of private (or equivalent). Over half of Porton Down veterans had been in military service for less than three years when they first went to Porton Down. Of the military and demographic factors examined in this study, the only clear difference between the two cohorts was that Porton Down veterans had a longer duration of military service. Fewer Porton Down than non-Porton Down veterans stayed for less than two years (2% (438/18 145) v 16% (2771/17 587)) and more stayed for 10 or more years (28% (5043) v 18% (3117)) (table 1).⇓ The median duration of military service was 6.2 years (interquartile range 4.2-11.4) for Porton Down veterans and 5.0 (2.1-7.5) for non-Porton Down veterans.
Characteristics of 18 276 Porton Down veterans and 17 600 non-Porton Down veterans. Figures are numbers (percentages) of veterans
The median interval between first and last test carried out at Porton Down was four days (interquartile range 1-8 days), and median number of days on which tests were performed was two (1-4).14 For 69% (12 601/18 276) of the Porton Down veterans, the first recorded visit to Porton Down was in the 1940s or 1950s (table 2)⇓. The type of test could be determined for 95% (17 303) of veterans and, of these, 91% (16 686) were in at least one test involving a chemical. Fifty eight per cent of veterans (10 539) were in at least one test involving a vesicant, 20% (3597) a nerve agent, and 65% (11 925) another chemical group (neither vesicant nor nerve agent) (table 2), with considerable overlap (fig 1)⇓.⇓ There were eight specific chemicals for which there were records of at least 1000 Porton Down veterans having been tested: three vesicants (sulphur mustard, Lewisite, and nitrogen mustard), one nerve agent (sarin), two lachrymators (CS and CR), and two anti-nerve agent pharmaceutical chemicals (pralidoxime and atropine) (table 2).⇓ The median number of tests per veteran was five for vesicants, one for nerve agents, and three for other chemicals.14

Fig 1 Overlap of exposure groups in 16 686 Porton Down veterans (excludes 1590 not recorded as exposed to any chemical)
{kind=link}
Summary of exposures in 18 276 Porton Down veterans, 1941-89
After a median follow-up of over 40 years (median 43.2 (interquartile range 31.4-51.0) for Porton Down and 43.7 (31.9-51.1) for non-Porton Down veterans), 40% (n=7306) of Porton Down and 39% (6900) of non-Porton Down veterans were notified as dead (table 1).⇑ All cause mortality in both groups was less than in the general population, with variation by branch of the services (table 3)⇓.
All cause mortality in Porton Down veterans and non-Porton Down veterans compared with national mortality rates according to service at enlistment. Standardised mortality ratios (95% confidence intervals) adjusted for calendar year and age group
All cause mortality in the Porton Down veterans was higher than that of the comparison group (rate ratio 1.06, 95% confidence interval 1.03 to 1.10, table 4),⇓ particularly in deaths not registered in the UK (1.26, 1.09 to 1.46). For UK deaths, we compared mortality in 12 groups of underlying causes (table 4).⇓ In four groups, there was a significant excess: infectious and parasitic (1.57, 1.07 to 2.29), genitourinary (1.46, 1.04 to 2.04), circulatory (1.07, 1.01 to 1.12), and external (non-medical) (1.17, 1.00 to 1.37) causes. There was a significant deficit for in situ, benign, and unspecified neoplasms (0.60, 0.37 to 0.99).
Cause specific mortality in Porton Down veterans compared with non-Porton Down veterans. Rate ratios (95% confidence intervals) with and without adjustment for age group and calendar period
When we restricted analysis to veterans with two or more years of service, the all cause mortality rate ratio was similar (1.07, 1.03 to 1.10). Rate ratios for all cause mortality were also examined by time since first test (table 5)⇓. The overall excess mortality relative to non-Porton Down veterans seemed to be present at all stages of follow-up examined.
All cause mortality in Porton Down veterans compared with non-Porton Down veterans according to time since first test. Rate ratios adjusted for five year age group and five year calendar period
Figures 2⇓, 3⇓, and 4⇓ present rate ratios according to chemical exposure group. The excess all cause mortality seen in the whole cohort was seen in most groups, as were several of the associations with cause specific mortality. Lewisite exposure was associated with cancers of the trachea, bronchus, and lung (1.19, 1.00 to 1.43). Table 6⇓ presents rate ratios for selected causes of death in subgroups with “high” exposure; in none was the estimate higher than the upper bound of the 95% confidence interval for the rate ratio for the exposure group as a whole.

Fig 2 Rate ratios for cause specific mortality in Porton Down veterans included in test(s) involving vesicant(s) compared with non-Porton Down veterans, adjusted for age and calendar period. Rate ratio estimates are represented by box with size inversely proportional to variance. Vertical dotted line shows estimate for all deaths. For clarity, only rows for major ICD chapter headings are presented
{kind=link}

Fig 3 Rate ratios for cause specific mortality in Porton Down veterans included in test(s) involving nerve agent(s) compared with non-Porton Down veterans, adjusted for age and calendar period. Rate ratio estimates are represented by box with size inversely proportional to variance. Vertical dotted line shows estimate for all deaths. For clarity, only rows for major ICD chapter headings are presented
{kind=link}

Fig 4 Rate ratios for cause-specific mortality in Porton Down veterans included in test(s) involving any other chemical(s) compared with non-Porton Down veterans, adjusted for age and calendar period. Rate ratio estimates are represented by box with size inversely proportional to variance. Vertical dotted line shows estimate for all deaths. For clarity, only rows for major ICD chapter headings are presented
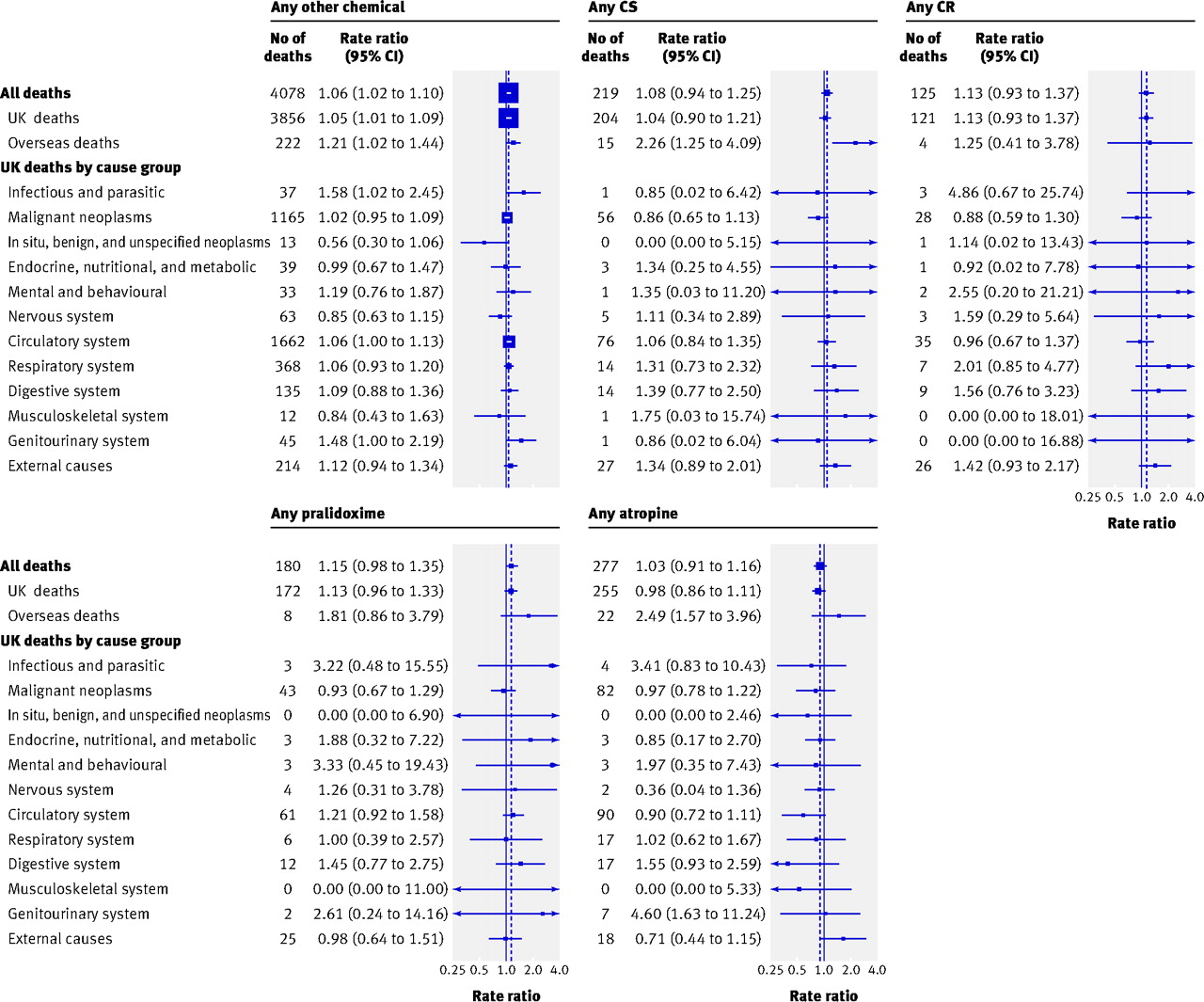{kind=link}
Mortality by selected underlying causes (ICD-10 code) for Porton Down veterans with high recorded levels of exposure to specific chemicals, relative to non-Porton Down veterans. Rate ratios adjusted for age group and calendar period (95% CI)
Discussion
Mortality in men in the armed forces who took part in tests at Porton Down from 1941-89 was slightly higher than that of similar veterans who did not take part (rate ratio 1.06). This excess was particularly evident in deaths from infectious and parasitic, circulatory, genitourinary, and external (non-medical) causes, as well as in deaths overseas for which no underlying cause was available. The excess in overseas deaths might be related to the longer duration of military service in the Porton Down veterans as they might have had more overseas military postings. Mortality from cancer was not increased, a similar finding to that for cancer morbidity.12 At the same time, overall mortality in Porton Down veterans was 12% lower than that of the general population. This is perhaps not surprising because these men had all met the selection criteria for military service; similarly low mortality has been found in other UK military cohorts, such as nuclear test veterans and submariners.17 18
Strengths and weaknesses
Our cohort is the largest reported to date with experimental exposure to chemical warfare agents and related chemicals and includes over 17 000 exposed veterans compared with 6720 and 1545 veterans studied in the United States.7 8 9 10 As well as collecting detailed exposure information13 14 we assembled a comparison group of similar veterans who did not attend Porton Down. The median duration of follow-up was over 40 years and should be sufficient for major long term risks to emerge.
Previous research
One possible explanation for the excess mortality is the chemical exposures received by the veterans or other aspects of the experience of visiting Porton Down. The best previous evidence for long term effects on health of chemical warfare agents relates to the vesicant sulphur mustard. Increased mortality from respiratory cancer was noted in US casualties from sulphur mustard in the first world war19 20 and in UK disability pensioners from the first world war who had been affected by sulphur mustard.21 UK workers who manufactured sulphur mustard in the second world war had raised mortality from malignant and non-malignant respiratory disease,22 and there were similar findings from Japan.23 Iranian authors associated sulphur mustard exposure in the Iran-Iraq war (1980-8) with respiratory disorders.24 There was no evidence of these effects in US navy veterans exposed experimentally to sulphur mustard.10 In Porton Down veterans with exposure to sulphur mustard, there was an 8% excess mortality from respiratory cancers and a 2% excess from non-malignant respiratory diseases, but these were not statistically significant and the findings in the “high” exposure subgroups were inconsistent. The probable explanation is that, whereas manufacturing workers accumulated months or years of exposure in repeated shifts, servicemen spent only days or weeks in these experimental programmes and the number of instances of exposure was fewer. Furthermore, in many of the tests the veterans wore protective equipment, which would have reduced their uptake of sulphur mustard.14
There have been few previous studies on the long term effects of these chemicals other than sulphur mustard.6 7 8 9 Although nitrogen mustard has been associated with leukaemias,25 mortality from lymphatic and haematopoietic cancers was not increased in this study. Our findings suggest that Lewisite exposure in Porton Down veterans might be associated with mortality from cancers of the trachea, bronchus, and lung.12
Interpretation
The associations we found between chemical exposure group and cause specific mortality are difficult to interpret. While they might represent effects of exposure at Porton Down, it is also possible that Porton Down and non-Porton Down veterans differed in ways that relate to mortality, leading to confounding. For example, the longer total military service of Porton Down veterans might imply differences in military factors such as overseas postings. We did not collect information about lifestyle factors that affect mortality, of which the most important is smoking. This limits interpretation, particularly of the excess of deaths attributed to circulatory causes, which are associated with smoking. Although the longer duration of military service in Porton Down veterans might indicate health related survival, the all cause mortality rate ratio was unchanged when we restricted analysis to those with two or more years of service.
The large number of outcomes and exposures means that some significant associations might have occurred by chance. On the other hand, we might have missed some genuine risks. Another potential limitation of this study, shared by all analyses of underlying cause of death, is that it is most informative about diseases with poor survival.
Summary
This large cohort study with detailed information on chemical exposure provides insights into the long term health of Porton Down veterans. Mortality was slightly higher than in non-Porton Down veterans but with the lack of information about other important factors, such as smoking or service overseas, we cannot attribute a small excess such as this to chemical exposures at Porton Down.
What is already known on this topic
Since the first world war, research programmes into chemical warfare agents and defences against them have involved experiments on members of the armed forces
Few studies have looked at the long term effects on their health
What this study adds
Mortality was slightly higher than expected in UK veterans of the programme at Porton Down
It was not possible to attribute the higher mortality to these chemicals in the absence of data on other risk factors, such as smoking
Notes
Cite this as: BMJ 2009;338:b613
Footnotes
We thank the research team who worked on the study (Monica Smith, Marita Lowry, Alison Howell, Margaret Chandler, Owen Rogers, the late Janice Hurwood, Sue Walker, Chris Shield, Nicola Pata, Kate Brockhurst, Steve Davies, Ian Palmer, and Madeleine Harwood); staff from the Ministry of Defence (MoD) who abstracted personnel data for the study; and Bianca De Stavola, David Cox, and Michael Hills for input on analytical methods. We also thank the following organisations for their contributions to different aspects of the study: Medical Research Council (MRC) Porton Down Research Liaison Group, Porton Down Veterans Support Group, MoD Veterans Policy Unit, Defence Science and Technology Laboratory at Porton Down, National Health Service Central Register, General Register Office for Scotland, Office for National Statistics, and Department for Work and Pensions. Figure 1 was originally generated with an applet developed by Peter Rodgers, University of Kent, and Stirling Chow, University of Victoria, Canada: www.cs.kent.ac.uk/people/staff/pjr/EulerVennCircles/EulerVennApplet.html. Figures 2-4 were originally plotted by Adrian Goodill, Cancer Epidemiology Unit, University of Oxford.
Contributors: KMV and LMC jointly led the study and are guarantors. All authors participated in the study design, plan of analysis, interpretation of the results, and drafting of the paper. LL carried out the statistical analyses.
Funding: This study was funded by the MRC with funds provided to it by the MoD. Additional funds were provided by the Department of Public Health and Nuffield College, University of Oxford. The MRC set up a liaison group to oversee the progress of the study. The MoD had no role in study design, analysis, and interpretation of data. The MoD facilitated access to its archives but had no role in deciding which data were abstracted. The MoD was sent a copy of the paper for factual comment but had no role in writing the paper or in the decision to submit for publication. The universities of Oxford and London are independent of both the MRC and the MoD.
Competing interests: None declared.
Ethical approval: The study was approved by the south east multicentre research ethics committee, the Defence Medical Services clinical research committee, and the Patient Information Advisory Group.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.