Risk of microalbuminuria and progression to macroalbuminuria in a cohort with childhood onset type 1 diabetes: prospective observational study
BMJ 2008; 336 doi: https://doi.org/10.1136/bmj.39478.378241.BE (Published 27 March 2008) Cite this as: BMJ 2008;336:697
- Rakesh Amin, consultant paediatric endocrinologist1,
- Barry Widmer, clinical resource coordinator1,
- A Toby Prevost, medical statistician2,
- Phillip Schwarze, clinical research fellow1,
- Jason Cooper, medical statistician3,
- Julie Edge, consultant paediatric endocrinologist4,
- Loredana Marcovecchio, clinical research fellow1,
- Andrew Neil, consultant diabetologist5,
- R Neil Dalton, consultant biochemist6,
- David B Dunger, professor of paediatrics and consultant paediatric epidemiologist1
- 1University Department of Paediatrics, Addenbrooke’s Hospital, Cambridge CB2 0QQ
- 2Department of Public Health and Primary Care, University of Cambridge, Cambridge CB2 0SR
- 3JDRF/Wellcome Trust Diabetes Inflammation Laboratory, Cambridge Institute for Medical Research, Cambridge CB2 0XY
- 4Department of Paediatrics, John Radcliffe Hospital, Oxford OX3 9DU
- 5Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford, Oxford OX3 7LJ
- 6WellChild Laboratory, King’s College London, Guy’s Hospital, London WC2R 2LS
- Correspondence to: D B Dunger dbd25{at}cam.ac.uk
- Accepted 25 January 2008
Abstract
Objectives To describe independent predictors for the development of microalbuminuria and progression to macroalbuminuria in those with childhood onset type 1 diabetes.
Design Prospective observational study with follow-up for 9.8 (SD 3.8) years.
Setting Oxford regional prospective study.
Participants 527 participants with a diagnosis of type 1 diabetes at mean age 8.8 (SD 4.0) years.
Main outcome measures Annual measurement of glycated haemoglobin (HbA1c) and assessment of urinary albumin:creatinine ratio.
Results Cumulative prevalence of microalbuminuria was 25.7% (95% confidence interval 21.3% to 30.1%) after 10 years of diabetes and 50.7% (40.5% to 60.9%) after 19 years of diabetes and 5182 patient years of follow-up. The only modifiable adjusted predictor for microalbuminuria was high HbA1c concentrations (hazard ratio per 1% rise in HbA1c 1.39, 1.27 to 1.52). Blood pressure and history of smoking were not predictors. Microalbuminuria was persistent in 48% of patients. Cumulative prevalence of progression from microalbuminuria to macroalbuminuria was 13.9% (12.9% to 14.9%); progression occurred at a mean age of 18.5 (5.8) years. Although the sample size was small, modifiable predictors of macroalbuminuria were higher HbA1c levels and both persistent and intermittent microalbuminuria (hazard ratios 1.42 (1.22 to 1.78), 27.72 (7.99 to 96.12), and 8.76 (2.44 to 31.44), respectively).
Conclusion In childhood onset type 1 diabetes, the only modifiable predictors were poor glycaemic control for the development of microalbuminuria and poor control and microalbuminuria (both persistent and intermittent) for progression to macroalbuminuria. Risk for macroalbuminuria is similar to that observed in cohorts with adult onset disease but as it occurs in young adult life early intervention in normotensive adolescents might be needed to improve prognosis.
Introduction
In adults with type 1 diabetes microalbuminuria is an early marker of structural renal disease1 and a risk factor for the development of macroalbuminuria.2 The presence of macroalbuminuria is associated with subsequent development of end stage renal disease and increased coronary mortality.3 4 After about 18 years of diabetes the cumulative prevalence of microalbuminuria and macroalbuminuria is 34%5 and 15%,5 6 respectively. Regression to normoalbuminuria occurs in 31-58% of adults with microalbuminuria six to eight years after onset of microalbuminuria5 6 and relates to modifiable factors such as glycaemic control, blood pressure, and lipid concentrations.5 6
In people with childhood onset type 1 diabetes, the cumulative prevalence of microalbuminuria is around 12-25% after five to 10 years of diabetes.7 8 9 10 11 12 Variability in these outcomes could be explained by differences in study design and bias from factors such as regression towards the mean.
The Oxford regional prospective study is a population based inception cohort of children with type 1 diabetes designed to determine prospectively the natural course of microalbuminuria during childhood and adolescence.13 Initial data indicated a cumulative prevalence of microalbuminuria of 40% after 11 years of diabetes, and this was predicted by poor glycaemic control but not by blood pressure.13 The prognostic value of microalbuminuria for progression to macroalbuminuria has not been adequately determined in a childhood cohort. We report on data from this study after up to 19 years of follow-up and focus on predictors for the development of microalbuminuria and macroalbuminuria.
Methods
Oxford regional prospective study
The Oxford regional prospective study was established in 1986.13 The study identified children aged under 16 in the Oxford Health Authority over a 10 year period from the St Bartholomew’s Oxford diabetes register and recruited children within three months of diagnosis. Case ascertainment for the register was over 95%.14 Parent gave written consent and children gave verbal assent. From 1986 to 1997, 91% (n=527) of eligible children were recruited at a mean age 8.8 (SD 4.0) years. To date the dropout rate is 9.6%. Parents gave written consent and children gave verbal assent. Mean duration of follow-up to date is 9.8 (3.8) years. Only 4% of the participants have been followed up for under three years, and 9% have over 15 years’ follow-up. In agreement with individual physicians, microalbuminuria was treated with angiotensin converting enzyme inhibitors or β blockers in those aged over 18 with persistent microalbuminuria or hypertension, or both.
Annual assessments
Research nurses assessed participants annually from the first year of diagnosis and recorded height, weight, blood pressure, and collected three consecutive early morning (first void) urine specimens for the measurement of albumin:creatinine ratio. We did not use urine specimens from girls who were menstruating (to avoid artificially high albumin concentrations). Blood samples were collected for centralised measurement of glycated haemoglobin (HbA1c).
Definition of microalbuminuria
Microalbuminuria was defined as a urinary albumin:creatinine ratio 3.5-35 mg/mmol in males and 4.0-47 mg/mmol in females in at least two consecutive early morning urine samples collected during the annual assessment (corresponding to an overnight albumin excretion rate of 20-200 μg/min and an albumin:creatinine ratio of 2.4 and 2.2 standard deviations above the geometric mean in normal male and female adolescents, respectively13). We collected an average of 2.8 urine samples per participant per year. Three urine samples were collected in 84% of all annual assessments and two samples collected in 16%.
Persistent microalbuminuria was defined as the presence of microalbuminuria at every subsequent annual assessment. In those with persistent microalbuminuria, diagnosis was based on two years of follow-up in 49% and over two years in 51%. Intermittent microalbuminuria was defined as a positive result during an annual assessment followed by regression to normoalbuminuria, then recurrence of microalbuminuria at a later date. Transient microalbuminuria was defined as regression of microalbuminuria to normoalbuminuria with no reoccurrence. Macroalbuminuria was defined as an albumin:creatinine ratio >35 mg/mmol in males and >47 mg/mmol in females.
Clinical investigations
We measured blood pressure with a random zero sphygmomanometer (Hawksley, UK) with appropriately sized cuffs on the non-dominant arm, with participants sitting and the arm supported, after a period of rest. We recorded blood pressure as the mean of two measurements to the nearest 2 mm Hg at Korotkoff sounds 1 and 5.
Albumin assay—Until 1994 urine samples were stored at −20°C and after this time at −70°C. Albumin was measured centrally by a double antibody enzyme linked immunosorbent assay (ELISA). The coefficient of variation within and between assays was 6% and 12%, respectively.
Creatinine concentration—Creatinine was measured with a modified Jaffe method (Unimate 7, Roche Diagnostic Systems, Switzerland) on a Cobas Mira (Roche Diagnostic Systems, Switzerland) automated spectrophotometer. The coefficient of variation was 2% at 2.2 mmol/l.
Glycated haemoglobin (HbA1c)—We initially measured HbA1c with electrophoresis (Ciba Corning Diagnostics, UK) and then used high performance liquid chromatography (DIAMAT; Bio-Rad, Hemel Hempstead, UK). The relation between the two methods was carefully evaluated and has been described previously.13 The coefficient of variation within batches for chromatography was 2.2% and 1.3% at a level of 9.8% and 10.1%, respectively. The coefficient of variation between batches was 3.5% and 2.2% at 5.6% and 10.1%, respectively. The normal range was 4.3-6.0%.
Statistical methods
As excretion of urinary albumin varies greatly within individuals and three consecutive measurements tend not to be normally distributed, we averaged three results from each participant with the geometric mean. The distributions of these yearly geometric means for the whole cohort were not normally distributed and were log transformed and analysed on this scale. All data were summarised as means for each patient. We analysed time, blood pressure, and HbA1c as continuous variables; these were normally distributed. Smoking status and antihypertensive treatment were analysed as dichotomised variables because data on actual number of cigarettes smoked and type of drug were unavailable. By definition microalbuminuria and macroalbuminuria status are binary measures and were therefore analysed as dichotomised variables. We compared groups with unpaired Student’s t tests and compared frequencies using χ2 tests. We used a life table method to calculate the cumulative prevalence (defined as the overall estimate of the total number of cases in the cohort after a given time) of microalbuminuria and macroalbuminuria and a log rank test to compare cumulative prevalence between groups, based on follow-up ending September 2005.
A Cox’s proportional hazard regression model was used to evaluate the relative contribution of covariates to the risk of developing microalbuminuria and macroalbuminuria, with duration of diabetes as the time covariate. Other variables included in the model were mean HbA1c concentrations, sex, blood pressure, smoking, and age at diagnosis of diabetes. We used a stepwise backward selection, with the significance level for inclusion of 5% and exclusion of 10%, and did not consider any interactions. Potential problems with the results from a Cox model may arise if participants with an albumin:creatinine ratio near the lower limit of the definition for microalbuminuria cross this level because of random measurement error or regression to the mean. Therefore, we used the same methods for sensitivity analyses, using alternative cut off values.
We used SPSS version 11.5 for all analyses. P<0.05 was considered as significant for each test, but given that many tests were undertaken we also applied a second more conservative P value of <0.01 to give a more cautious interpretation. Data are shown as means (SD) unless otherwise stated.
Results
Cumulative prevalence of microalbuminuria
Of 527 participants, 135 (26%) met the study definition of microalbuminuria after 5182 patient years of follow-up (fig 1)⇓. The cumulative prevalence of microalbuminuria was 25.7% (95% confidence interval 21.3% to 30.1%) after 10 years of diabetes and 50.7% (40.5% to 60.9%) after 19 years. The mean age at onset of microalbuminuria was 16.1 (4.3) years. Compared with those without, those with microalbuminuria were older (19.5 (4.0) v 18.4 (4.7), P=0.01), had had diabetes for longer (10.5 (3.4) years v 9.6 (3.8) years, P=0.009), and had higher mean lifetime HbA1c concentrations (10.8% (1.7%) v 9.5% (1.4%), P<0.001) and higher HbA1c concentrations at diagnosis of diabetes (10.9% (1.8%) v 9.7% (1.8%), P<0.001). The probability of microalbuminuria increased progressively with increasing quarters of HbA1c (fig 2, log rank test P<0.001)⇓.

Fig 1 Numbers with microalbuminuria and progression to macroalbuminuria up to September 2005
{kind=link}
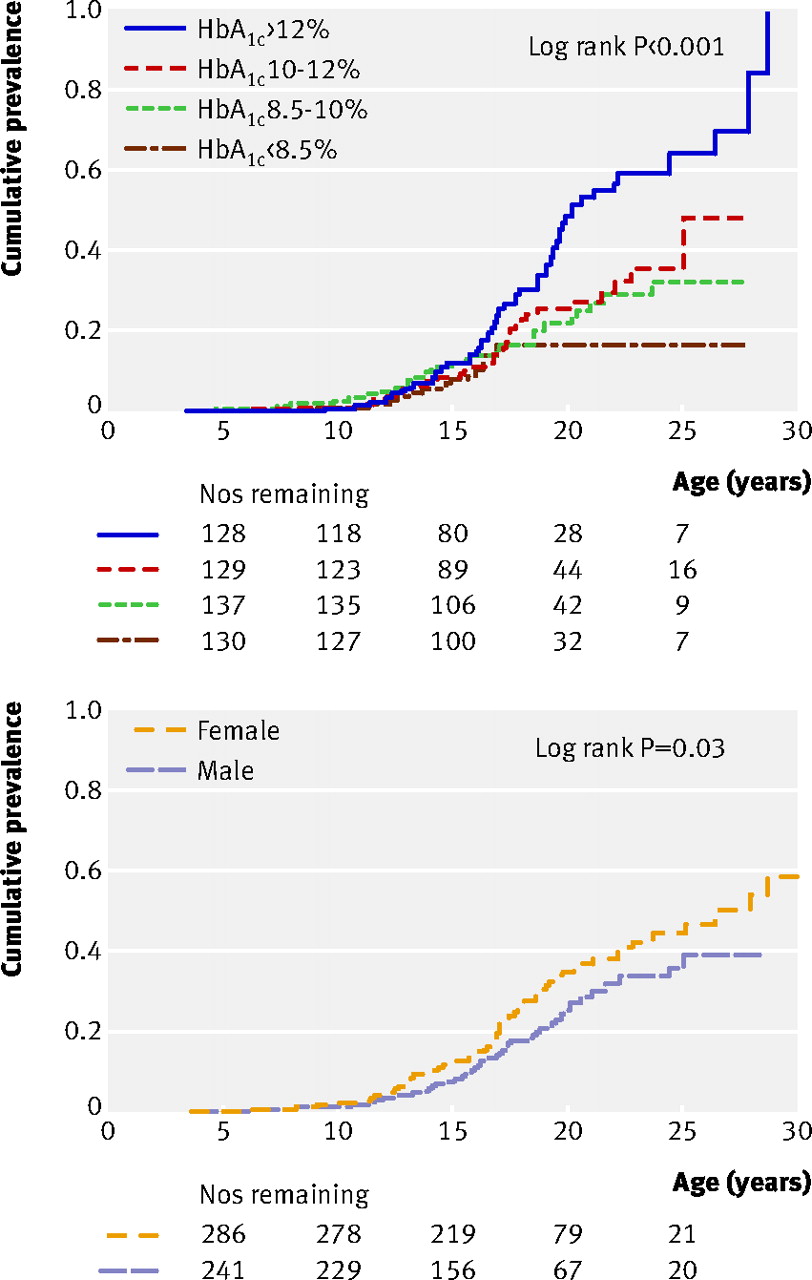
Fig 2 Kaplan-Meier survival curves showing cumulative prevalence of developing microalbuminuria (135 events) across age in 527 children with type 1 diabetes, 1986-2005, in relation to quarters of mean lifetime HbA1c concentrations (top) and sex (bottom)
{kind=link}
More females than males developed microalbuminuria (n=72 (53%) v n=63 (47%), fig 2, log rank test P=0.03).⇑ This sex difference was not explained by differences in age, HbA1c concentrations, or duration of diabetes.
As previously reported,13 in those with a diagnosis of diabetes before the age of 5 (n=27), compared with those with a diagnosis at ages 5-11 (n=64) and after 11 (n=44), there was a longer interval between age at diagnosis to first appearance of microalbuminuria (8.8 (3.8) years v 7.7 (3.8) v 5.5 (3.3) years, P=0.01, with or without adjustment for HbA1c concentrations) (fig 3)⇓. After 10 years of diabetes, in the group with a diagnosis before the age of 5 compared with the two other groups, cumulative prevalence of microalbuminuria was lower (age at diagnosis <5 years: 17.4% (9.8% to 25.0%); 5-10 years: 28.7% (21.7% to 35.7%); >11 years: 28.9% (20.5% to 37.3%); log rank test P=0.035). After 15 years of diabetes, however, cumulative prevalence was similar in the three groups (<5 years: 43.0% (25.0% to 61.0%); 5-11 years: 45.7% (33.3% to 58.1%); and >11 years: 40.8% (27.2% to 54.4%); log rank test P=0.1, fig 3).⇓

Fig 3 Kaplan-Meier survival curve showing cumulative prevalence of development of microalbuminuria (135 events) across duration of diabetes in 527 children with type 1 diabetes, 1986-2005, in relation to age at diagnosis of diabetes
{kind=link}
Predictors for development of microalbuminuria
Of previously described predictors, significant unadjusted correlates of microalbuminuria were poor glycaemic control (1.35, 1.24 to 1.47, P<0.001—that is, a 35% increased risk for a 1% rise in HbA1c), female sex (1.43, 1.02 to 2.01, P=0.04), diastolic blood pressure (1.02, 1.00 to 1.04, P=0.04), and younger age at diagnosis of diabetes (1.06, 1.01 to 1.10, P=0.01). Non-contributory variables included systolic blood pressure (1.01, 0.99 to 1.02, P=0.17) and history of smoking (1.32, 0.89 to 1.94, P=0.23).
In a Cox model, the only modifiable adjusted predictor for the development of microalbuminuria was poor glycaemic control (table 1)⇓. Female sex was also associated with microalbuminuria but blood pressure, history of smoking, and age at onset of diabetes did not contribute to the model (table 1).⇓ When we excluded data from those with two consecutive annual urine samples with positive results, rather than three, the results were materially unaffected. In a separate Cox model, sensitivity analysis with adjustment of the definition of microalbuminuria (reduced lower limits for the definition of microalbuminuria by 0.5 mg/mmol and 1.0 mg/mmol) showed that outcomes were not dissimilar to when the standard definition was used (table 1).⇓
Cox model* with sensitivity analysis with adjusted definition of microalbuminuria showing adjusted, modifiable predictors for the development of microalbuminuria in 527 children with type 1 diabetes followed for up to 19 years, after correction for duration of diabetes. Figures are hazard ratios (95% confidence intervals) with P values
Course of microalbuminuria
Of the 135 participants with microalbuminuria, 65 (48%) developed persistent microalbuminuria, 17 (13%) had intermittent microalbuminuria, and 53 (39%) had transient microalbuminuria (fig 1), giving a cumulative prevalence of regression to the normoalbuminuric range of 51.9% (42.3% to 61.5%) after 4.9 years after the onset of microalbuminuria.⇑ Classification of persistent microalbuminuria was based on results of four or more annual urine collections in 43% of participants. All those with intermittent microalbuminuria had more than three further years of follow-up and had time periods ranging from 1.0 to 7.2 years in which they were normoalbuminuric. Those with transient microalbuminuria had a median follow-up of 6.8 (4.2) years after their last urine sample with a positive result, with 51 (96%) having more than three years of follow-up.
Duration of diabetes was greater in participants with persistent rather than with intermittent and transient microalbuminuria (table 2)⇓. Overall mean HbA1c concentrations were highest in those with persistent microalbuminuria and lowest in those with transient microalbuminuria, and this was most apparent after the onset of microalbuminuria (table 2)—that is, lower concentrations of HbA1c after the onset of microalbuminuria were associated with regression of microalbuminuria (hazard ratio 1.21, 1.07 to 1.54—that is, a 21% increased occurrence of regression for a 1% lowering of HbA1c, after adjustment for duration of diabetes).⇓ There were no significant differences in age at onset of microalbuminuria or in sex ratio between the three groups.
Characteristics of participants with childhood onset type 1 diabetes according to microalbuminuria status (see text for definitions). Figures are mean (SD) years unless stated otherwise
Development of macroalbuminuria
Eighteen participants developed macroalbuminuria (13% of those with microalbuminuria, 3% of total cohort) giving a cumulative prevalence of 13.9% (12.9% to 14.9%) after 3.2 (2.9) years after onset of microalbuminuria (fig 1).⇑ Median age at development of macroalbuminuria was 18.5 (5.8) years and duration of diabetes was 10.0 (4.0) years.
Those who developed macroalbuminuria had higher mean HbA1c concentrations compared with the rest of the cohort (table 3)⇓ and higherblood pressure after the development of microalbuminuria (systolic 126.5 mm Hg (15.6 mm Hg) v 118 mm Hg (13.8 mm Hg), P=0.009; diastolic 85.6 mm Hg (9.9 mm Hg) v 79.4 mm Hg (8.4 mm Hg), P=0.03).
Characteristics of participants with type 1 diabetes with and without macroalbuminuria. Figures are mean (SD) years unless stated otherwise
Significant unadjusted correlates of macroalbuminuria were poor glycaemic control (1.47, 1.18 to 1.82, P<0.001—that is, a 47% increased risk for a 1% rise in HbA1c), persistent microalbuminuria (39.10, 11.33 to 135.21, P<0.001), intermittent microalbuminuria (15.78, 4.24 to 60.62, P<0.001), and systolic blood pressure (1.02, 0.99 to 1.06, P=0.04). Non-contributory variables included female sex (1.00, 0.39 to 2.54, P=0.89), diastolic blood pressure (1.04, 0.99 to 1.09, P=0.09), history of smoking (1.83, 0.69 to 4.81, P=0.27), and younger age at diagnosis of diabetes (1.05, 0.94 to 1.17, P=0.56).
The modifiable adjusted predictors for progression from microalbuminuria to macroalbuminuria were poor glycaemic control and persistent and intermittent microalbuminuria (table 4).⇓ Factors not contributing to outcome were sex, blood pressure, history of smoking, and age at diagnosis of diabetes. Sensitivity analysis with adjustment of the definition of macroalbuminuria (reduced lower limits for the definition of macroalbuminuria by 5 mg/mmol and 10.0 mg/mmol) showed that predictors remained as strong as when we used the standard definition (table 4).⇓
Cox model* with additional sensitivity analysis with adjusted definition of macroalbuminuria showing adjusted modifiable predictors for development of macroalbuminuria in 527 children with type 1 diabetes followed for up to 19 years, after correction for duration of diabetes. Figures are hazard ratios (95% confidence intervals) with P values
Intervention with antihypertensive medication
Twenty (15%) participants with microalbuminuria (13 with persistent microalbuminuria and seven with intermittent microalbuminuria and hypertension) were treated with an angiotensin converting enzyme inhibitor or a β blocker. Age at start of drug treatment was 21.9 (3.8) years and subsequent follow-up was 5.1 (4.0) years. In participants with microalbuminuria who received treatment compared with those who did not there were no significant differences in HbA1c concentrations or history of smoking or systolic and diastolic blood pressure before treatment.
Seven (35%) participants receiving treatment progressed to macroalbuminuria (and these were all previously categorised as having persistent microalbuminuria) compared with 11 (10%) with microalbuminuria not receiving treatment (χ2=9.5, P=0.002). In these two groups there were no difference in mean HbA1c concentrations during treatment (11.1% (1.9%) v 11.0% (2.4%), P=0.77) or history of smoking, though there was a non-significant trend towards higher systolic (134.4 mm Hg (13.2 mm Hg) v 121.0 mm Hg (15.3 mm Hg), P=0.15) and diastolic (90.0 mm Hg (9.3 mm Hg) v 82.5 mm Hg (9.5 mm Hg), P=0.17) blood pressure.
Discussion
In this inception cohort of people with childhood onset type 1 diabetes, the cumulative prevalence of microalbuminuria was 25.7% and 50.7% after 10 and 19 years of diabetes, respectively, and the cumulative prevalence of macroalbuminuria was 13.9% after 19 years.
Comparisons with other studies
For microalbuminuria, the cumulative prevalence was significantly higher than that observed in the adult only inception cohort (from the Steno clinic), in which prevalence was nearly 34% after 18 years of follow-up and similar glycaemic exposure5 (table 5)⇓. This prevalence is greater than previously reported in longitudinal childhood studies,9 10 11 but those previous studies were clinic based, with variable duration of diabetes at inclusion compared with our cohort, in which all participants were recruited at diagnosis, case ascertainment was high, and dropout rates low. Despite differences in prevalence of microalbuminuria, the prevalence of macroalbuminuria of 13.9 was similar to that in the adult inception data from the Steno clinic but occurred at a much earlier age (table 5).5 ⇓ No comparable data exist for children, although previous small clinic based studies indicate a prevalence of macroalbuminuria of 7-32%.7 12 15
Comparison of Oxford regional prospective study childhood inception cohort with adult inception cohort from the Steno clinic (Hovind et al5). Figures are mean (SD) years unless stated otherwise
Implications of poor glycaemic control
Glycaemic control was unequivocally linked to the risk of microalbuminuria and progression to macroalbuminuria. Although generally HbA1c concentrations in our study were above currently accepted goals for glycaemic control, there was no threshold below which microalbuminuria did not occur. Both baseline and more recent lack of glycaemic control predict risk of microalbuminuria,5 16 and follow-up data from the diabetes control and complications trial showed that previous intensive treatment of patients with diabetes and near normal glycaemia has an extended benefit in delaying progression of diabetic nephropathy.17 Collectively these data indicate that both remote and more recent glycaemic control might be equally important, and therefore in children the goal should be improvement of control from the onset of diabetes.
Recent reports suggest a declining incidence of diabetic nephropathy with improvements in glycaemic control.18 The 2002 Diabetes UK audit, however, indicated that 48% of adolescents were not achieving HbA1c concentrations less than 9%,19 and the Hvidore study also recently reported that HbA1c concentrations during adolescence were disappointing.20 We contend that the poor levels of glycaemic control reflect the high ascertainment in our study and that they are an accurate reflection of HbA1c concentrations during adolescence, particularly during transition to adult clinics in the UK.21
Other predictors of microalbuminuria
Unlike our childhood onset cohort, in adult onset cohorts prevalence of microalbuminuria is greater in men (table 5).5 ⇑ The reason for this reversal in sex risk from childhood to adulthood onset disease is unclear but might be explained by data indicating a role for sex steroids in renal damage associated with diabetes22 and associations between hyperandrogenism and abnormalities in the growth hormone insulin-like growth factor I axis in adolescent girls with microalbuminuria.23
Cumulative prevalence of microalbuminuria at the end of follow-up was unaffected by age at diagnosis, though in those with a diagnosis before the age of 5 there was a longer interval to first appearance of microalbuminuria. Other data indicate that before the onset of microalbuminuria, the annual rate of rise of urinary albumin excretion increases after the age of 11.24 Although detailed Tanner staging of puberty was unavailable in the current cohort, collectively these data indicate that exposure to well characterised physiological and psychosocial changes during the pubertal years might be important in the timing of the first appearance of microalbuminuria21 23 25 but not the cumulative prevalence.
Transient microalbuminuria
In the current cohort, in over half of the participants with microalbuminuria it was defined as “transient” or “intermittent” about 4.9 years after the onset of microalbuminuria. This contrasts with rates of regression of 31% in the inception cohort from the Steno clinic5 but is similar to the 58% six years after onset of microalbuminuria reported in another study in adults.6 Definition of regression of microalbuminuria is complicated by regression to the mean and duration of follow-up. Some studies have used categorical novel definitions of regression, suggesting that 50% reduction in albumin excretion would minimise confounding effects of variability in urinary albumin excretion,6 but such definitions are still based on duration of follow-up. Our data indicate that people who have microalbuminuria in one year but become normoalbuminuric in the next year might be at risk of recurrence in one to seven years. Thus rate of regression must depend on duration of follow-up, and further follow-up data from the Oxford study might reveal more cases of intermittent microalbuminuria among those currently categorised as transient.
Risk for macroalbuminuria
Perhaps more important is the early detection of risk for microalbuminuria and progression to macroalbuminuria, which could result in more accurate identification of people in need of intervention. In the current study, only 18 patients developed macroalbuminuria, so predictors and comparison with the remainder of the cohort should be interpreted with caution. Our data indicate that the only modifiable predictor for the development of macroalbuminuria was poor glycaemic control. Both persistent and intermittent microalbuminuria are important predictors in the transition to macroalbuminuria in children, and these factors are robust after sensitivity analyses. In contrast with findings from studies in adults, those taking angiotensin converting enzyme inhibitors actually had higher rates of progression to macroalbuminuria. Only 20 patients had started this treatment, however, and our study was not designed to determine the effects of treatment. There could also be ascertainment bias as few participants with microalbuminuria were treated and age at onset of treatment was late. This negative result could also be the result of small sample size, variable duration of follow-up, differences in treatment protocols between clinics, and differences in blood pressure. The efficacy of angiotensin converting enzyme inhibition needs to be explored in a controlled prospective intervention study in this age group.
Limitations of study
We collected annual urine samples on three consecutive days rather than spaced through the year, but this relates to the practicalities of running a long term field study. Annual assessment of urinary albumin:creatinine ratio, however, is based on the average of three measurements, which reduces measurement error and regression to the mean. The requirement of the study to have measurements once a year could also reduce the effect of regression to the mean as true changes emerging over a year are less likely to be overturned by measurement error.
The use of Cox models is associated with inherent problems, as it requires a strict cut off point for the definition of microalbuminuria and macroalbuminuria. We used sensitivity analyses, with lower limits for the definitions of microalbuminuria and macroalbuminuria, to assess any influence of measurement error on thresholds. Predictors were essentially unchanged, validating the outcomes and indicating a continuum of risk with increasing urinary albumin excretion within the normal range for the development of microalbuminuria and in the microalbuminuric range for the development of macroalbuminuria.
Finally, we did not have sufficient data on variables such as insulin regimens, which may have had a confounding effect on the outcome.
Conclusion
There is higher cumulative prevalence of microalbuminuria with predominance of risk in females in people with childhood onset type 1 diabetes compared with those who had adult onset disease. Our data indicate that microalbuminuria might not be persistent in over half of cases. As this depends on duration of follow-up, further cases of intermittent microalbuminuria might occur with longer follow-up of those with “transient” microalbuminuria. The probability of progression to macroalbuminuria is remarkably similar to that in adult onset disease, but it occurs at an earlier age and in people with both intermittent and persistent microalbuminuria. Therefore, as the ultimate prognosis might be worse in someone with childhood onset rather than adult onset type 1 diabetes, there is a need to consider earlier intervention strategies in those diagnosed with diabetes during childhood.
What is already known on this topic
Microalbuminuria and macroalbuminuria are associated with the development of end stage renal disease in adult onset type 1 diabetes and might be predicted by poor glycaemic control and higher blood pressure
What this study adds
In those with childhood onset type 1 diabetes, microalbuminuria occurred more frequently and was more common in females but the only modifiable predictor was high HbA1c concentrations
Modifiable predictors of macroalbuminuria were high HbA1c concentrations and both persistent and intermittent microalbuminuria
Risk for macroalbuminuria is similar to adult onset type 1 diabetes but as it occurs in young adult life , early intervention during adolescence might be needed to improve prognosis
Footnotes
We acknowledge the study field workers, the laboratory assistance of Angie Watts and Dot Harris, the Barts-Oxford study field workers, paediatricians, physicians, and diabetes nurse specialists in the Oxford region.
Oxford regional prospective study steering committee: D B Dunger, R N Dalton, J Fuller, E A M Gale, H Keen, M Murphy, H A W Neil, R J Young, and T Konopelska-Bahu.
Oxford regional prospective study members: J Edge, John Radcliffe Hospital, Oxford; H A W Neil and David Matthews, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, Oxford; R A F Bell and A Taylor, Horton General Hospital, Banbury; A Mukhtar, B P O’Malley, B R Silk, and E H Smith, Kettering District Hospital, Kettering; R D M Scott, King Edward VII Hospital, Windsor; F M Ackland, C J Fox, and N K Griffin, Northampton General Hospital; N Mann, H Simpson, P Cove Smith, and M Pollitzer, Royal Berkshire Hospital, Reading; R S Brown and A H Knight, Stoke Mandeville Hospital, Aylesbury; J M Cowen and J C Pearce, Wexham Park Hospital, Slough.
Contributors: RA wrote the paper and was the main statistical analyser. BW coordinated collection of clinical samples and data. ATP and JC were statistical advisers. PS and LM cowrote the manuscript. JE and AN were local ORPS investigators. RND coordinated collection and analysis of urine samples. DBD led the ORPS steering committee, cowrote the manuscript, gave statistical advice, and is guarantor.
Funding: Diabetes UK, the Juvenile Diabetes Research Foundation, the Wellcome Trust, NIHR Cambridge Biomedical Research Centre.
Competing interests: None declared.
Ethical approval: District ethics committees.
Provenance and peer review: Not commissioned; externally peer reviewed.