The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysisCommentary: patients, preferences, and evidence
BMJ 2000; 320 doi: https://doi.org/10.1136/bmj.320.7246.1380 (Published 20 May 2000) Cite this as: BMJ 2000;320:1380
Abstract
Objective: To investigate the impact of patients' preferences for the treatment of atrial fibrillation, by using individualised decision analysis combining probability and utility assessments into a decision tree.
Design: Observational study based on interviews with patients.
Setting: Eight general practices in Avon.
Participants: 260 randomly selected patients aged 70–85 years with atrial fibrillation.
Main outcome measures: Patients' treatment preferences regarding anticoagulation treatment (warfarin) after individualised decision analysis; comparison of these preferences with treatment guidelines on the basis of comorbidity and absolute risk and compared with current prescription.
Results: Of 195 eligible patients, 97 participated in decision making using decision analysis. Among these 97, the decision analysis indicated that 59 (61%; 95% confidence interval 50% to 71%) would prefer anticoagulation treatment—considerably fewer than those who would be recommended treatment according to guidelines. There was marked disagreement between the decision analysis and guideline recommendations (kappa =0.25 or less). Of 38 patients whose decision analysis indicated a preference for anticoagulation, 17 (45%) were being prescribed warfarin; on the other hand, 28 (47%) of 59 patients were not being prescribed warfarin although the results of their decision analysis suggested they wanted to be.
Conclusions: In the context of shared decision making, individualised decision analysis is valuable in a sizeable proportion of elderly patients with atrial fibrillation. Taking account of patients' preferences would lead to fewer prescriptions for warfarin than under published guideline recommendations. Decision analysis as a shared decision making tool should be evaluated in a randomised controlled trial.
The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis
- Joanne Protheroe, Wellcome entry level training fellowa,
- Tom Fahey, senior lecturer (tom.fahey{at}bristol.ac.uk)a,
- Alan A Montgomery, MRC health services research training fellowa,
- Tim J Peters, reader in medical statisticsb
- a Division of Primary Health Care, Department of Social Medicine, University of Bristol, Bristol BS8 2PR
- b Department of Social Medicine, University of Bristol
- Epidemiology Unit, London School of Hygiene and Tropical Medicine, London WC1E 7HT
- Correspondence to: T Fahey
- Accepted 15 March 2000
Abstract
Objective: To investigate the impact of patients' preferences for the treatment of atrial fibrillation, by using individualised decision analysis combining probability and utility assessments into a decision tree.
Design: Observational study based on interviews with patients.
Setting: Eight general practices in Avon.
Participants: 260 randomly selected patients aged 70–85 years with atrial fibrillation.
Main outcome measures: Patients' treatment preferences regarding anticoagulation treatment (warfarin) after individualised decision analysis; comparison of these preferences with treatment guidelines on the basis of comorbidity and absolute risk and compared with current prescription.
Results: Of 195 eligible patients, 97 participated in decision making using decision analysis. Among these 97, the decision analysis indicated that 59 (61%; 95% confidence interval 50% to 71%) would prefer anticoagulation treatment—considerably fewer than those who would be recommended treatment according to guidelines. There was marked disagreement between the decision analysis and guideline recommendations (kappa =0.25 or less). Of 38 patients whose decision analysis indicated a preference for anticoagulation, 17 (45%) were being prescribed warfarin; on the other hand, 28 (47%) of 59 patients were not being prescribed warfarin although the results of their decision analysis suggested they wanted to be.
Conclusions: In the context of shared decision making, individualised decision analysis is valuable in a sizeable proportion of elderly patients with atrial fibrillation. Taking account of patients' preferences would lead to fewer prescriptions for warfarin than under published guideline recommendations. Decision analysis as a shared decision making tool should be evaluated in a randomised controlled trial.
Introduction
Atrial fibrillation is an independent risk factor for developing stroke. Randomised trials have established that anticoagulation with warfarin is associated with a relative reduction in risk of stroke of 68%.1 Community based studies that estimated the prevalence of atrial fibrillation, however, show underdiagnosis and undertreatment.2 3 Commentators from general practice attribute poor uptake in clinical practice to a lack of representativeness of patients enrolled in clinical trials. In particular, patients managed in primary care may find what are deemed to be “minor” side effects from anticoagulation more problematic than do highly selected patients in clinical trials.4 5
Decision analysis is a form of shared decision making that explicitly combines the probabilities of events resulting from treatment decisions with quantitative estimates of the patient's perceptions (utilities) regarding the consequences of treatment.6 The increasing computerisation in general practices, along with the development of user friendly software, means that utility assessment with decision analysis is a realistic aim for decision making with individual patients.7
Qualitative research has established that patients' health beliefs are important factors in determining whether they accept or decline anticoagulation treatment for atrial fibrillation.8 We examined the impact of patients' preferences, measured by utility assessment, on treatment choices and compared this method of decision making with evidence based recommendations based on age and comorbidity or absolute risk of stroke.9–11
Methods
Selection of participants
We invited 17 general practices to take part in the study, of which 13 accepted. Owing to time constraints, only the first eight practices on an unordered list were included. We identified patients with atrial fibrillation by means of a diagnostic code on the practices' computer records and repeat prescriptions for digoxin. We used random number tables to select patients aged between 70 and 85 years. We sampled 30 or 40 patients per practice, depending on the list size, yielding a total sample size of 260 patients. In each practice the list of sampled patients was shown to the general practitioners, and unsuitable patients were excluded (see the figure on the BMJ's website). We sent letters and an information sheet to the remaining patients inviting them to take part in the study. We then telephoned patients to arrange an interview (with JP) at their practice; written consent was obtained at the start of the interview.
Decision analysis
Details of each participant's risk factor profile were abstracted from practice records and verified with the participant. Absolute annual risks of a thromboembolic event were derived from a literature search and tailored to each individual participant according to his or her age and comorbidity (table 1). The relative risk reduction and the probability of side effects if warfarin treatment was given were also obtained from the literature, as was the likelihood of functional independence after a stroke (table 1). The treatment alternatives and their possible consequences were then mapped out by means of a decision tree (fig 1). The nine health states (outcomes) from the decision tree were shown on laminated cards to the participant, who then ranked them in order of preference. Utilities for each health state were elicited using the “time trade-off” method, which quantifies the length of time in perfect health that is viewed by the patient to be equivalent to a given period of ill health (box). Participants were also asked to complete a short questionnaire to assess how they felt about the interview process.
Example of time trade-off method
To assess the utility of the health state “treated with warfarin, experienced side effects, has had cardiovascular accident, unaffected afterwards” (see fig 1) in a 75 year old woman
The patient is asked to choose between two alternatives: living in the health state in question until age 80; or living in perfect health for a shorter length of time. The options are presented on laminated sheets, and the age to which the patient could live in perfect health is varied until she is unable to choose between the two alternatives. Let us suppose that she regards living until age 77 in perfect health as “equivalent to” living until age 80 in the health state in question—that is, she would be willing to give up three of her remaining five years of life to have perfect health. Utility of the health state in question is then calculated as:
1-(number of years willing to give up/(80-current age))
This would be 1 - (3/5)=0.4, with 0.4 representing the value that this patient places on this state of health.
Values of probabilities used at various chance nodes in decision tree (see fig 2)
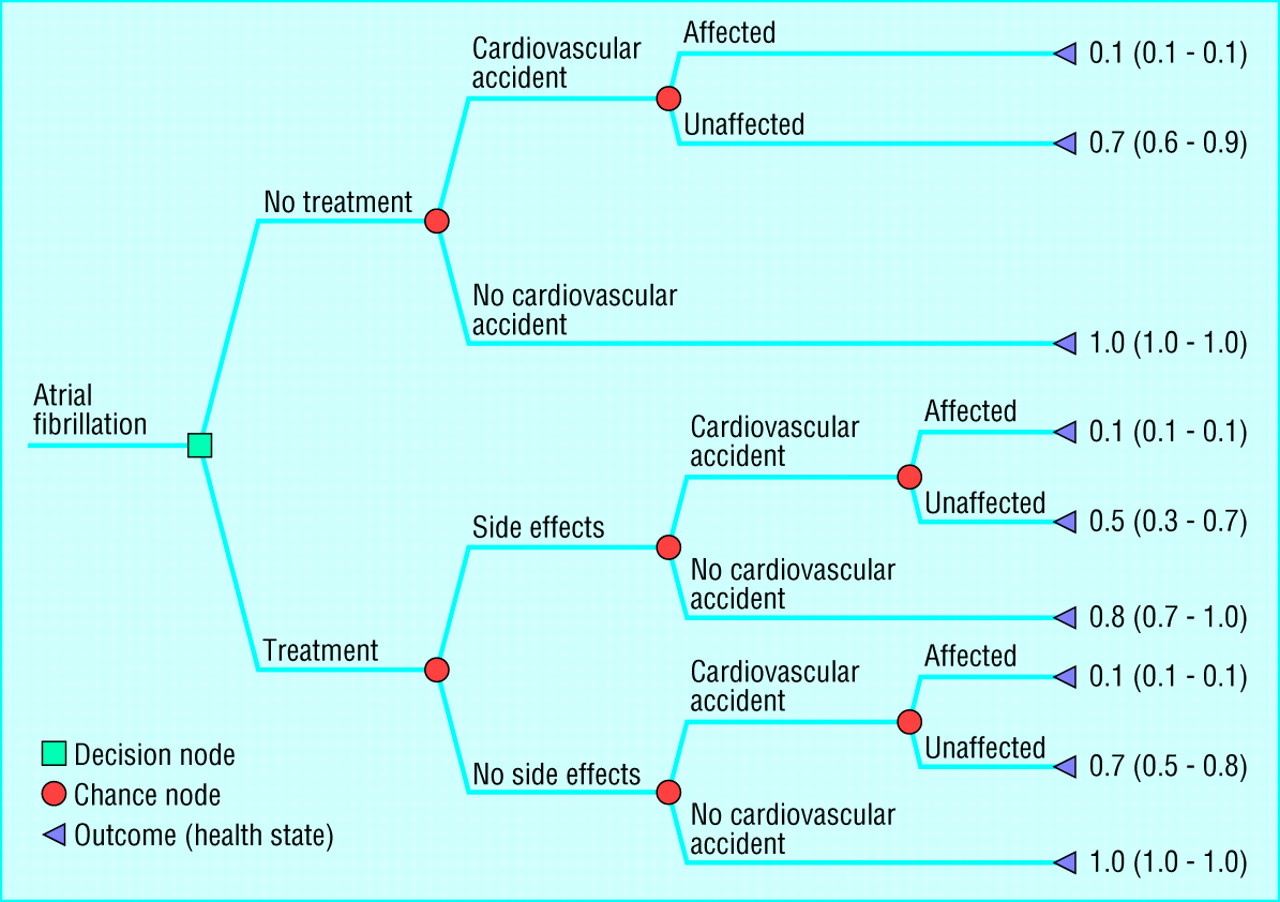
Decision tree of health states resulting from having atrial fibrillation with utility values (median (interquartile range)) for each health state
{kind=link}
Data analysis
The probabilities (risks) and utilities were assigned to each individual's decision tree. These were then multiplied and summed to give expected utility values for the two main branches of the tree (treatment and no treatment). After this, a participant was to accept treatment if the expected utility of “treatment” exceeded that of “no treatment.” In the primary analysis, the probability of “any” side effects was used; the probabilities for “major” and “minor” side effects were incorporated into a sensitivity analysis.
Each participant's preference about warfarin treatment from the decision analysis was compared with recommendations by using two sets of published criteria based only on comorbidity and age.9 11 The first of these was from a consensus conference, which included recommending treatment for all patients aged over 75 years, regardless of risk factors.9 The second recommendation was based on absolute annual risk for all patients, using risks derived from the literature as in table 1. In this study, warfarin treatment was assumed to be recommended if the participant's absolute annual risk was greater than 5%—this is consistent with recent guidelines based on absolute risk.11 The result of the decision analysis was also compared with whether the participant was receiving anticoagulation treatment at the time of interview.
All these comparisons were performed by using crude percentages of disagreements between the classifications, both overall and by type of disagreement. The level of agreement that would be expected by chance was corrected for usingκstatistics.15 Ethical approval was obtained from our local research ethics committee before the start of the study.
Results
Representativeness
In all, 97 participants completed the decision analysis. table 2 shows the characteristics of these participants. The sex ratio was similar to that for the original sample of 260 patients (55% female). The participants were also comparable in several respects to those recruited in the five randomised controlled trials evaluating the use of warfarin or aspirin in atrial fibrillation, except that women were underrepresented in the trials.1
Characteristics of study participants (n=97). Values are numbers of participants unless stated otherwise
Proportions recommended for warfarin according to various criteria
Individuals' utility values varied little within each health state (fig 1). According to the decision analysis, 59 of the 97 (61%; 95% confidence interval 50% to 71%) participants preferred treatment with warfarin; the corresponding figures for the other two recommendations were 89 (92%; 84% to 96%) for the consensus conference 9 and 70 (72%; 62% to 81%) when based on absolute risk.11

Levels of disagreement between treatment preferences based on decision analysis and recommendations of treatment guidelines from a consensus conference9 and absolute risk
{kind=link}
Comparison of decision analysis with recommendations and current treatment
The primary comparison of the decision analysis based on “any” side effects with the other recommendations shows a high level of disagreement (fig 2). Moreover, most of the discrepancies are “false positives”—for example, of the 38 participants whose decision analysis indicated that they preferred not to be treated with warfarin, 87% would have been recommended for treatment according to the consensus conference's guidelines (fig 2). As the chance of minor side effects is closely similar to that of “any” side effects, the results of this part of the sensitivity analysis are not shown. Indeed, even though the risk of major side effects is considerably lower, using this probability in the calculations for the decision analysis had no appreciable effect on the results (fig 2). The measure of agreementκ statistic) for treatment preferences based on decision analysis and corrected for chance compared with the consensus guidelines and absolute risk recommendations were 0.09 and 0.25 when “any” side effects were considered and were 0.05 and −0.04 respectively when major side effects were considered, indicating “poor” levels of agreement.
Of the 38 participants whose decision analysis indicated that they preferred not to be treated with warfarin, 17 (45%) were in fact being prescribed warfarin. Of the remaining 59 participants, 28 (47%) were not being prescribed warfarin—that is, contrary to their decision.
Questionnaire responses
Altogether, 82 participants stated a preference to be involved in shared decision making about their medical care; 67 reported current involvement. Ninety participants thought that the decision analysis interview could be performed in general practice, by either their general practitioner or a practice nurse. When asked whether they found it unsettling to discuss the possibility of having a stroke or side effects from treatment, 73 said “no,” 22 said “a little,” and 2 said that they found it “very” unsettling.
Discussion
Interpretation of findings
When incorporated by means of decision analysis, patients' preferences could have an important impact on treatment choice in elderly patients, with nearly 40% of patients with atrial fibrillation in this study preferring not to receive anticoagulation. Furthermore, when the results of decision analysis are compared with guidelines based on absolute risk of stroke, there is marked disagreement (fig 2). Guidelines ignoring patients' preferences would recommend treatment for a higher proportion of patients.
A large proportion of elderly people were either unwilling or too unwell to participate in shared decision making—at least in the context of a research study (see figure on the web). This may act as a barrier to using any form of shared decision making tool in clinical practice.16 On the other hand, questionnaire responses from those who participated in decision analysis accord with previous findings that decision analysis is well accepted by patients, and most (85%) interviewees would prefer to be involved in clinical decision making.17
Table 2 shows that apart from an underrepresentation of women, the participants in this study were not substantially different from participants in clinical trials for treatment of atrial fibrillation.1 This suggests that reluctance to apply results of randomised trials may not be justifiable purely on the basis of differences in patients' characteristics.4
Comparison with guidelines
Guidelines for anticoagulation in atrial fibrillation based on absolute risk or clinical criteria have been widely promulgated.9 11 Glasziou and Irwig equate one death from intracranial haemorrhage with prevention of four thromboembolic strokes and suggest that when the annual risk of stroke exceeds 2% the benefits start to outweigh the potential harm induced by anticoagulation treatment.10 This form of absolute risk assessment has been used as the criterion for judging evidence based treatment in the community.9 11 Wide concern has been expressed that when such criteria are used, atrial fibrillation is being undertreated in elderly people.2 3 18 The results from this study suggest that treatment choice among elderly people is more complex than simply applying absolute risk standards of treatment. Factors relating to individual patients have been described and attributed as one of the reasons for poor uptake of anticoagulation treatment.19 It seems that among patients who are willing and able to participate in shared decision making, individual preferences and probabilities may combine to make some patients more averse to the consequences of anticoagulation than to the consequences of atrial fibrillation. The findings of this study suggest that guidelines for the management of atrial fibrillation should be modified to incorporate patients' preferences in treatment decisions, particularly with regard to the consequences of anticoagulation treatment.20 21
Previous studies
Qualitative research has established the importance of patients' preferences as a major factor in determining choice of treatment.8 A randomised trial evaluating the efficacy of anticoagulation treatment shows that quality of life is substantially reduced when patients experience even “minor” side effects.22 Sensitivity analyses in the current study show that variation in the severity and likelihood of the side effects for individual patients has an impact on treatment choice and confirms the importance of eliciting patients' preferences.23
Decision analysis is usually used as a means of implementing evidence in practice, with preferences being elicited at a group level.6 With the development and increasing sophistication of computer software, however, individual decision analysis is likely to be more common in the future.16 This study suggests that elicitation and participation by means of decision analysis will enable patients to become more involved in the decision making process. Decision aids improve knowledge and reduce decisional conflict without increasing anxiety.24 A recent randomised trial showed that an audiobooklet about atrial fibrillation improved patients' understanding of the benefits and risks of treatment choices.17 Though promising, most decision aids usually involve imparting knowledge to patients; they do not evaluate patients' own values about the consequences of treatment.25 To date there has only been one randomised controlled trial of personalised decision analysis showing that it did influence clinical decision making in individuals.26 If decision analysis is to be used as a shared decision making tool, it will require “protected” time for the patient in the same way that videos and patient information leaflets are currently used as shared decision making tools. Some software can elicit individual patients' preferences and can be used on a personal computer.
Study limitations
There are certain constraints with utility assessment, primarily in achieving a balance between keeping the decision tree as simple as possible and including all the relevant patient centred outcomes. It is possible to elicit and then aggregate complex utility states (such as severity of side effects), but this may be at the expense of better understanding for the patient and doctor.27 In this study, therefore, separate utility values were not elicited for major and minor side effects; rather, all potential side effects were represented together.
All interviews were conducted face to face by the same researcher, and interviewer bias cannot be excluded in such circumstances. More objective utility assessment may be possible in the near future using interactive computer programs.16 Lastly, only eight of the original 17 practices participated in this study, and in those practices only half of the eligible patients took part in decision analysis (see figure on the web). Responses in these individuals may be systematically different from those that might have been given by non-respondents, and further replication of these findings is required.
Conclusion
In this observational study, eliciting preferences and performing decision analysis does seem to have important implications for clinical practice. Decision analysis as a shared decision making tool, and in particular its impact on patients' knowledge, satisfaction, and uptake of and adherence to anticoagulation, should be examined in a randomised controlled trial.24
What is already known on this topic
Qualitative research has established the importance of patients' preferences as a major factor in determining choice of anticoagulation treatment in patients with atrial fibrillation
Decision analysis is a form of shared decision making that explicitly combines the probabilities of events resulting from treatment decisions with quantitative estimates of the patients' preferences
What this study adds
This study shows that eliciting patients' preferences and performing decision analysis has a major impact on an individual's preference for anticoagulation treatment
Evaluation of decision analysis as a shared decision making tool, and its impact on patients' knowledge, satisfaction, uptake, and adherence to anticoagulation treatment, should be examined in a randomised controlled trial
Acknowledgments
We thank all 13 Avon practices and 260 patients for participating in this study. Both the division of primary health care and the department of social medicine are part of the MRC Health Services Research Collaboration.
Contributors: The study was conceived and designed by TF and TJP. Practices and patients were recruited by JP. Interviews with all the patients were conducted by JP. AAM and JP performed the statistical analyses with input from TF and TJP. TF and JP drafted the paper with contributions from AAM and TJP. JP and TF are the guarantors.
Footnotes
Funding This study was funded as part of a Wellcome entry level training fellowship for JP. TF receives some funding from an NHS R&D primary care career scientist award
Competing interests None declared.
References
Commentary: patients, preferences, and evidence
- Liam Smeeth, clinical research fellow (liam.smeeth{at}lshtm.ac.uk)
- a Division of Primary Health Care, Department of Social Medicine, University of Bristol, Bristol BS8 2PR
- b Department of Social Medicine, University of Bristol
- Epidemiology Unit, London School of Hygiene and Tropical Medicine, London WC1E 7HT
This paper shows that where good evidence exists decision analysis is a feasible way of incorporating patients' values and preferences into clinical decisions. The fact that only about half of the patients who were approached participated should not be viewed critically: decision analysis will not suit all patients.
Patients' choices of treatment frequently disagreed with both consensus guidelines and with guidelines based on an assessment of absolute risk. Overall, the proportion of people who preferred warfarin treatment was lower than the proportion for whom such treatment is recommended by either of the guidelines. Patients' preferences did not, however, all act in the same direction. Considerable numbers of people preferred warfarin treatment, even though this was not recommended by either of the guidelines. Given good information, the participants were able to weigh up the benefits and drawbacks of the intervention and make a personal choice.
The study shows that when patients are actively involved in clinical decision making their preferences may strongly influence treatment decisions. Successfully involving patients in clinical decisions requires good information. The most reliable source of information about the effects of interventions comes from sufficiently large, well conducted randomised controlled trials.1 By definition, however, randomised controlled trials measure the effects of randomly assigned interventions. Randomisation is the key process by which bias and confounding are minimised. Can the importance of patients' preferences be reconciled with the benefits of randomisation? This issue has been discussed in depth elsewhere.2–4 The best study design that has been proposed to tackle this dilemma uses a two stage approach.5 During the first stage, participants are randomised to two groups: a “random” group and a “preference” group. In the second stage, participants in the random group are randomised a second time to the two interventions being compared in the trial. Participants in the preference group are given a free choice between the two interventions being assessed. This design has the unique advantage of being able to measure the influence of patients' preferences on the estimate of the treatment effect. Clearly there will be times when patients' (or clinicians’) preferences for one treatment or another are sufficiently strong to preclude randomisation.
The study by Protheroe et al shows that shared decision making can be achieved when high quality relevant research evidence about clinical questions is available to patients and clinicians. Good clinical practice can then be informed by the evidence; it may not always follow the evidence.
Footnotes
Competing interests None declared.
 A figure showing the study profile appears on the BMJ's website
A figure showing the study profile appears on the BMJ's website