Scientific, ethical, and logistical considerations in introducing a new operation: a retrospective cohort study from paediatric cardiac surgery
BMJ 2000; 320 doi: https://doi.org/10.1136/bmj.320.7243.1168 (Published 29 April 2000) Cite this as: BMJ 2000;320:1168
- Catherine Bull, senior lecturer in paediatric cardiology (C.Bull{at}gosh-tr.nthames.nhs.uk),
- R Yates, consultant paediatric cardiologist,
- D Sarkar, registrar in paediatric cardiology,
- J Deanfield, professor of cardiology,
- M de Leval, professor of cardiac surgery.
- Correspondence to: C Bull
- Accepted 12 April 2000
Abstract
Objective: To review the initial impact on mortality of infants with congenital heart disease of a new surgical technique that is now taken for granted.
Design: Retrospective cohort study.
Setting: A tertiary paediatric cardiology centre.
Subjects: 325 consecutive neonates with simple transposition of the great arteries admitted before, during, and after the preferred management changed from the Senning operation to the arterial switch (1978-98); and 100 consecutive neonates requiring a different neonatal open heart operation that did not change in that period.
Main outcome measures: Mortality before and early after operation reconstructed sequentially as the series evolved and retrospectively once the series was complete; actuarial survival associated with the different treatment strategies.
Results: For both the transposition and the comparison group, early mortality in 1998 was lower than in 1978. During that period, however, there was a phase temporally related to the adoption of the switch operation in which early mortality for transposition increased. Actuarial survival of recent patients with “intention to treat” with arterial switch is superior to those with intention to treat with the Senning operation, as predicted when the switch operation was first adopted.
Conclusions: A period of increased hazard for individual patients may occur when a specialist community, a particular unit, and an individual surgeon are all learning a new technique concurrently. Obtaining informed consent during this time of uncertainty is helped by clarity about the objectives of treatment and availability of relevant local and international data.
Introduction
The introduction of a new management strategy to a group of patients for whom a long established treatment is also available has scientific, ethical, and logistical repercussions, particularly when the two treatments have different profiles of early and late hazards or benefits.
We examined the consequences of an institutional decision to replace a physiological repair (the Senning procedure) with an anatomical repair (the arterial switch operation) for the treatment of “simple” transposition of the great arteries. Transposition presents with cyanosis in the neonatal period: the aorta emerges from the right ventricle and the pulmonary artery from the left ventricle. Treatment for transposition from 1959 to the mid-1980s involved atrial baffle procedures (Mustard and Senning), which require the right ventricle to sustain systemic output long term. The arterial switch gradually became the favoured treatment for transposition of the great arteries during the 1980s 1 2: the great arteries are reconnected to the appropriate ventricle, and the coronary arteries are separately transferred to the “new” aorta. Unlike a physiological repair, this procedure must be performed in the neonatal period. Thus the “switch” involved the performance of a more difficult operation on younger patients in the anticipation of long term benefit.
In 1985 Macartney (from our unit) developed a detailed actuarial model incorporating what was objectively known and subjectively understood about the relative short, medium, and long term hazards of the Senning and switch strategies.3 This model clearly showed the implications of anxieties about the late hazard on projections of longevity after a Senning and formed the basis of an institutional decision to change from a Senning to a switch protocol.
We aimed to review the precision of predictions of the 1985 model compared with current data and examine whether it was correct in supporting the change to the switch. We also reviewed the impact of the changeover on early mortality for simple transposition of the great arteries against a background of general improvements in neonatal surgical and non-surgical management occurring in the same era.
Patients and methods
In our hospital the Senning replaced the Mustard operation in 1978 and was performed until 1992. Switch-type operations have been performed since 1979 for patients with transposition associated with complex intracardiac lesions (in 1979-85, 18 such operations were performed, with 5 early deaths). In January 1986 we performed our first elective switch operation for simple transposition of the great arteries.
This study involves all 325 consecutive patients with simple transposition who arrived alive aged <21 days in our hospital from August 1978 to February 1998 and who had all their subsequent treatment—including balloon atrial septostomy—under our care. This represents about 75% of patients with simple transposition seen at our hospital. Such patients would have undergone an elective Senning operation at age 4-12 months during the “Senning era” or an elective switch operation before age 21 days during the “switch era.”
For each case, the original management plan (“intention to treat”) and the operation they actually underwent was determined from hospital records. Each patient was given two “sequence” numbers: a transposition number (1 to 325), according to birth order; and a Senning number (1 to 144) or a switch number (1 to 181), according to their intention to treat and date of operation. The whole series could be divided into three periods: era 1 (before the first switch—transposition 1-117); era 2 (during the overlap between Senning and switch procedures—transposition 118 to 221); and era 3 (after the last Senning procedure—transposition 222 to 325). Four surgeons were involved in the management of these patients, only one of whom operated throughout the experience. Patient follow up is complete to the time of writing.
Early postoperative death was defined as death within 30 days of surgery; in analyses by intention to treat, patients who died before surgery were also regarded as early deaths. Sequential changes in early outcome over the experience were explored prospectively (tracking) and retrospectively. Plots of cumulative mortality against sequence number allowed reconstruction of “current mortality” data case by case as the experience unfolded.4 Logistic regression models were used to summarise the same early mortality experience “retrospectively” when the series was complete. To allow for the possibility of a peak in mortality in the course of the experience, a quadratic function was used with the sequence number and the sequence number squared as covariates in the models. Actuarial data were analysed with Kaplan-Meier methodology. The BASIC program in which Macartney's model of 1985 was prepared was rewritten as an Excel spreadsheet, and hazards corresponding to currently available data were entered.
To examine the background influence on outcome of the many subtle changes in medical and surgical management of neonates from 1978 to 1998, the outcomes of the 100 consecutive neonates arriving with total anomalous pulmonary venous drainage were reviewed. Such patients also present with cyanosis and require surgery as neonates, but their surgical strategy did not change.
Results
Intention to treat
For 144 patients the intention on arrival was to treat with the Senning procedure, and for 181 the intention was to treat with the switch. However, 19 patients (6%) died before definitive surgery (Senning, 16; switch, 3). Though some of these patients died very early from perinatal hypoxia or in association with balloon atrial septostomy, eight patients for whom the intention to treat was with the Senning procedure died outside the perinatal period while awaiting surgery. Such patients might not have died with a switch protocol.
Changes of plan
Eight patients who had surgery did not have the operation originally intended. All were managed early during the switch experience and the intention to treat was with the switch operation. In one patient perinatal neurological complications contraindicated early open heart surgery and the Senning procedure was performed at 14 months. In seven patients, the surgical approach was changed because of the intraoperative findings, mainly of “difficult” coronary anatomy. Six of these had a neonatal Senning operation (1 early and 1 late death), and 1 had an atrial septectomy (1 death).

Cumulative mortality along the series (1978-98) for infants who had a Senning operation, a switch operation, all infants with simple transpositions including preoperative death, and all infants with total anomalous pulmonary venous drainage (see methods section for explanations of eras)
{kind=link}
Early surgical outcomes
The Senning procedure was performed in 135 patients (8 early deaths (6%)) and a switch in 170 patients (23 early deaths (14%)). Figure 1 uses a cumulative mortality plot to reconstruct the picture of “current” mortality on data available case by case as the experience unfolded. Mortality after the Senning procedure remained essentially unchanged over the experience—the slope of the cumulative mortality plot is steady. In contrast, the early mortality for the switch varied over the experience—the slope of the cumulative mortality plot is steeper in era 2 than in era 3 (fig 1 (top)).
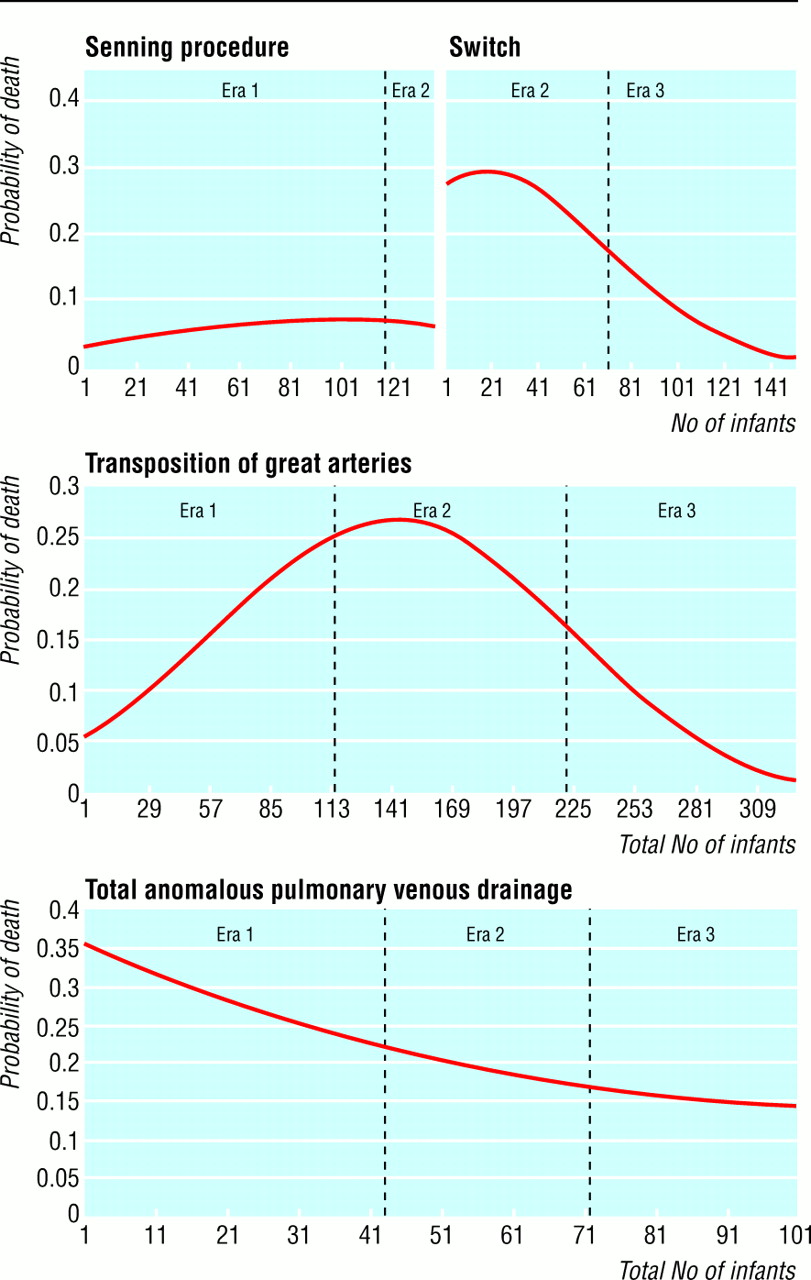
Logistic regression models. Senning and switch model the mortality of infants who had these operations. Transposition of the great arteries and total anomalous pulmonary venous drainage show mortality for the whole series by diagnosis (see methods section for explanations of eras)
{kind=link}
Figure 2 shows logistic regression models of the mortality pattern over the whole experience generated once the series was complete. Although for both transposition and total anomalous pulmonary venous drainage the mortality was lower in 1998 than in 1978, mortality for total anomalous pulmonary venous drainage dropped gradually whereas mortality for transposition rose before falling again in era 3.
Late mortality
Figure 3 shows the actuarial survival curves for intention to treat with the Senning procedure and with the switch. The late attrition in the Senning curve is greater than with the switch, and the late hazard may even be increasing with age. Deaths after the Senning procedure related to baffle obstruction, arrhythmia, and systemic ventricular dysfunction.5 The follow up of the switch patients is shorter, however, and problems, perhaps affecting the coronary arteries, may still emerge.6

Actuarial survival of patients with intention to treat with the Senning procedure and the switch. The switch data are stratified by era. Switch survival in era 3 is superior to Senning survival (P=0.04). The values in parentheses show the numbers of patients alive at time of procedure and at 5 year intervals (see methods section for explanations of eras)
{kind=link}

Top: Model published in 1985 contrasting estimates of the survival curves for the normal population with patients committed to a Senning operation at age 1 month with a 2% operative mortality and an annual late hazard of 2% and for patients committed to a switch operation at birth with a 40% early mortality and a 0.3% annual late hazard. Bottom: Current model, with normal survival as above. The Senning operation is assumed to take place at age 4 months and be associated with a hazard of 16% (including preoperative deaths) and an annual late hazard of 0.7%. The switch is assumed to be done at age 2 weeks and be associated with a 6.2% mortality (including preoperative deaths) and a 0.16% annual late hazard
{kind=link}
Models
Figure 4 contrasts the projections generated in 1985 using assumptions based on local and published data then available with those generated using data from this series. Inevitably the pattern of mortality beyond 15 years is generated entirely by extrapolation. The 1985 model applied a constant late annual hazard of 2% after the Senning procedure and 0.3% after the switch. Under these assumptions, the anticipated life expectancy (the average age at death) with the Senning procedure was 36.4 years and with the switch was 38.1 years, even if the operative mortality for the Senning was 2% and for the switch 40%. From the current data, the estimate of early mortality related to intention to treat with the Senning procedure is 16% (largely accounted for by preoperative deaths), with a late hazard estimate of 0.7% annually. For the current switch model, total preoperative and perioperative mortality in era 3 was 6.2%, and the late hazard estimated from the whole experience was 0.16% annually. This estimates a life expectancy of 62.6 years for simple transposition with intention to treat with the switch and 46.6 years for intention to treat with the Senning procedure, compared with 71.4 years for the normal population used in both calculations.
Discussion
This study shows that the theoretical rationale based on life expectancy projections used to justify the change from a Senning to a switch policy has been corroborated by the outcomes obtained so far in practice. Comparisons incorporating both early and late hazard are crucial when new treatment approaches are being introduced, particularly in childhood. If early risk alone had been considered, the arterial switch operation (which had a higher early mortality when first introduced) might have been abandoned. The data now available show that the arterial switch is a better option than the Senning procedure for newborns with simple transposition of the great arteries and emphasise the impact of late hazard on survival of a cohort of patients. It follows that the first survivors of the switch operation were the first beneficiaries of the superior treatment. However, the new strategy, though currently associated with a lower operative risk, accounted for a period of increased hazard for patients with simple transposition when it was first introduced. Limitation of the risk associated with changeover is clearly of both ethical and logistical importance.
Justification of change in strategy
Although comparisons incorporating early and late morbidity and mortality data are desirable, it is common for a new strategy with theoretical advantages to be introduced before the late outcomes of the old strategy have had time to emerge. In paediatric practice it is particularly common to have to make decisions involving extrapolations far beyond available data. Essentially Macartney's 1985 model concluded that a substantially higher operative mortality for the switch could still be associated with improved life expectancy for transposition, provided that the late hazard was small compared to the Senning procedure. This understanding, coupled with an appreciation of the persistently abnormal haemodynamics of the Senning procedure and the emergence of problems during follow up, 7 8 justified a change in surgical strategy. Data emerging during the last 12 years of this study period differ from the estimates in the 1985 model, but the treatment approach that it supported was appropriate. On the basis of current data, the average life expectancy after a switch will be 16 years longer than after a Senning operation.
Modelling techniques require clinicians to make explicit much of the data and subjective assessments they implicitly use in decision making. These assumptions are used both to build the models and to provide their working parameters; flaws in the assumptions will often be revealed as more data emerge. The most obvious problem with the 1985 model was its underestimation of the early mortality associated with the intention to treat with the Senning procedure by ignoring the attrition before the actual operation. To avoid inappropriate inferences being drawn, tracking even of two apparently “surgical” options should be by diagnosis and intention to treat rather than a naive comparison of two early postoperative mortalities.
Even when current data are used to provide the parameters, the predictions that the model offers for survival into middle age and beyond could be overoptimistic for both cohorts. The advent of coronary artery disease may prove a particular hazard for both cohorts.6
Radical changes in practice must be reviewed against a background of many more minor modifications in management; such changes presumably account for the gradual fall in mortality for total anomalous pulmonary venous drainage over the era. The transient increase in the early hazard for transposition of the great arteries associated with the changeover from a Senning to a switch policy is therefore representative of the learning curve for the new treatment.
Learning curves
Three separate components of the learning curve are discernible: the specialist community, the institution, and the individual surgeon learning the new technique. Whereas the three curves would be successive for a surgeon learning the arterial switch now, at the beginning of the switch experience the curves were overlapping and the outcomes worse. In high risk activities, such as paediatric cardiac surgery or aviation, strategies to minimise or compensate for misjudgments that occur during the learning process are vital.
The international specialist community—Reviewing the “grapevine” of the world experience of switch for simple and complex transposition to 1979, Jatene documented 89 operations with 54 deaths.9 At least for series beginning before mid-1985, outcomes of the switch were poor by current standards.10–16 Many reports dealing with the switch during the 1980s provide evidence of the international specialist community learning about the “biology” of the new operation. The specialist community now has rapid access to such information, but a bias to submit good results for publication will give an optimistic view of a new treatment. Contributing to multicentre databases opens up the potential to provide a constantly up to date picture of the learning curve nationally or internationally, but only if such databases are configured to capture the early results associated with a new treatment.
An individual institution—The specialist team within an institution also negotiates a learning curve. In our example, seven patients scheduled for a neonatal switch operation returned from the operation room having had an alternative procedure, usually because the coronary artery anatomy had been inadequately delineated preoperatively by the cardiologists. As in other series,16 crossover was associated with morbidity and mortality. A new surgical protocol is likely to have new information requirements and may alter the contribution of many of the team members.
An individual surgeon—The experience of a surgeon learning a new operation in which the steps of the operation are well described will be entirely different from the experience of tackling an operation which has only just been developed and for which therefore little or no reference material exists. Frameworks within which surgical trainees learn procedures exist, and formal guidelines for their adoption may limit the risk to patients during training. For a more established surgeon, apprenticeship arrangements are less ordered, but the value of operating along with another experienced surgeon has been emphasised.4 17
Management of innovation
A new treatment should ideally be introduced within an appropriate scientific, logistical, and ethical framework, but there is little momentum to progress towards more accountability in new surgery. Making such a process accountable could stifle innovation and impair the flexibility of surgeons to make creative decisions on the basis of a picture that emerges only in the operating room. At each new operation, however, a scientific hypothesis is being tested, and the need for “tracker” trials—designed for the context of fast changing technologies and guided by flexible protocols that allow for learning curves—is evident.18 Such trials should facilitate the identification of treatments that are performing poorly, as well as rejecting harmful new treatments, and should hopefully provide maximum information about which treatment is best, combining the benefits of randomised controlled trials with those of registers of new technologies.
What is already known on this topic
Many new operations are adopted outside a framework of formal ethical or scientific scrutiny
New treatments are usually judged by their early results, even if the treatment is meant to be a long term investment
Expressions of “current” mortality are difficult when outcomes are changing fast
Learning curves, particularly in paediatric cardiac surgery, are hard to accept
What this study adds
The study documents the superiority of an operation that had a higher early but lower late mortality than the operation that it was replacing
Implementation of this operation was associated with a transient increase in mortality while the international specialist community, the hospital team, and the individual surgeons learned about the new operation
Ethical issues are associated both with the decision to offer a new treatment and the informed decision to accept it. Clinical ethics committees could help to structure this process—and in doing so give the patient reassurance and the surgeon confidence—and clarify the medicolegal situation. A strategy for monitoring outcomes and possibly informal stopping rules could be agreed and scrutinised by such a committee. There are circumstances, particularly pertaining to decisions taken in early childhood, when crucial discussions cannot be evidence based. In our example, both a treatment whose outcomes were uncertain and some difficult issues of early and late hazard (and how these were valued) had to be communicated in accessible language. The ethical communication of an offer of a relatively new treatment is also complicated by the various ways of expressing “current” mortality (“series so far,” “last year,” “last 10”) that may give different estimates, particularly when mortality is changing rapidly over time. As a result it may be difficult to be honest with a patient or family without seeming evasive.
Logistical difficulties surround the introduction of a new treatment that minimises risk to patients while maximising the availability of the experience to the wider medical community. Ideally, institutions pioneering new treatments should have an acceptable record in related areas and have enough patients to enable rapid learning. This approach would see new strategies concentrated in a limited number of centres. Such centralisation and the possibility of having more than one specialist surgeon operating together could amplify the experience, while reducing the effect of an individual's learning curve. Both ideas, however, require movement of patients and some change of professional culture. Finally, an acceptable means of monitoring the change both institutionally and individually needs to be established so that institutional decisions and individual performance can be reviewed.
Conclusion
Many new operations are adopted outside a framework of formal ethical or scientific scrutiny. In our experience a new surgical strategy was accompanied by a learning curve while not only surgeons, but also the institution, adapted to the demands of the new treatment. Debate has made poor outcomes associated with learning less acceptable, both in the medical profession and among the general public. Frameworks must be developed that aim at maximising any benefit to a group of patients while minimising the risk to each individual.
Acknowledgments
We thank Adelaide Tunstill and Rebecca Clayton for their help in collecting the data and Fergus Macartney for his contribution to the original research question.
Contributors: CB initiated the formulation of the original study hypothesis, analysed the data, and was the principal author of the paper. RY initiated the research, collected the switch data, participated in data analysis, and helped to write the paper. DS collected and participated in analysis of the data on the Senning procedure and helped to write the paper. JD helped to interpret the data and to write and edit the paper. MdeL was involved in discussing core ideas and study design and contrib-uted to the interpretation of the data and to writing the paper. RY is the guarantor.
Footnotes
-
Funding None
-
Competing interests None declared.