Collaborative overview of randomised trials of antiplatelet therapy Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients
BMJ 1994; 308 doi: https://doi.org/10.1136/bmj.308.6921.81 (Published 08 January 1994) Cite this as: BMJ 1994;308:81
- Antiplatelet Trialists' Collaboration
- Correspondence to: APT Statistical Secretariat, ICRF/BHF/MRC Clinical Trial Service Unit, Nuffield. Department of Clinical Medicine,Radcliffe Infirmary, Oxford OX2 6HE, or APT Clinical Secretariat,Department of Clinical Neurosciences, Western General Hospital, Edinburgh EH4 2XU.
- Accepted 12 October 1993
Abstract
Objective: To determine the effects of “prolonged” antiplatelet therapy (that is, given for one month or more) on “vascular events” (non-fatal myocardial infarctions, non-fatal strokes, or vascular deaths) in various categories of patients.
Design: Overviews of 145 randomised trials of “prolonged” antiplatelet therapy versus control and 29 randomised comparisons between such antiplatelet regimens.
Setting: Randomised trials that could have been available by March 1990.
Subjects: Trials of antiplatelet therapy versus control included about 70 000 “high risk” patients (that is, with some vascular disease or other condition implying an increased risk of occlusive vascular disease) and 30 000 “low risk” subjects from the general population. Direct comparisons of different antiplatelet regimens involved about 10 000 high risk patients.
Results: In each of four main high risk categories of patients antiplatelet therapy was definitely protective. The percentages of patients suffering a vascular event among those allocated antiplatelet therapy versus appropriately adjusted control percentages (and mean scheduled treatment durations and net absolute benefits) were: (a) among about 20 000 patients with acute myocardial infarction, 10% antiplatelet therapy v 14% control (one month benefit about 40 vascular events avoided per 1000 patients treated (2P< 0.00001)); (b) among about 20 000 patients with a past history of myocardial infarction, 13% antiplatelet therapy v 17% control (two year benefit about 40/1000 (2P<0.00001)); (c) among about 10 000 patients with a past history of stroke or transient ischaemic attack, 18% antiplatelet therapy v 22% control (three year benefit about 40/1000 (2P<0.00001)); (d) among about 20 000 patients with some other relevant medical history (unstable angina, stable angina, vascular surgery, angioplasty, atrial fibrillation, valvular disease, peripheral vascular disease, etc), 9% v 14% in 4000 patients with unstable angina (six month benefit about 50/1000 (2P<0.00001)) and 6% v 8% in 16 000 other high risk patients (one year benefit about 20/1000 (2P<0.00001)).
Reductions in vascular events were about one quarter in each of these four main categories and were separately statistically significant in middle age and old age, in men and women, in hypertensive and normotensive patients, and in diabetic and non: diabetic patients. Taking all high risk patients together showed reductions of about one third in non-fatal myocardial infarction, about one third in non-fatal stroke, and about one sixth in vascular death (each 2P<0.00001). There was no evidence that non-vascular deaths were increased, so in each of the four main high risk categories overall mortality was significantly reduced. The most widely tested antiplatelet regimen was “medium dose” (75-325 mg/day) aspirin. Doses throughout this range seemed similarly effective (although in an acute emergency it might be prudent to use an initial dose of 160-325 mg rather than about 75 mg). There was no appreciable evidence that either a higher aspirin dose or any other antiplatelet regimen was more effective than medium dose aspirin in preventing vascular events. The optimal duration of treatment for patients with a past history of myocardial infarction, stroke, or transient ischaemic attack could not be determined directly because most trials lasted only one, two, or three years (average about two years). Nevertheless, there was significant (2P<0.00001) further benefit between the end of year 1 and the end of year 3, suggesting that longer treatment might well be more effective.
Among low risk recipients of “primary prevention” a significant reduction of one third in non: fatal myocardial infarction was, however, accompanied by a non-significant increase in stroke. Furthermore, the absolute reduction in vascular events was much smaller than for high risk patients despite a much longer treatment period (4.4% antiplatelet therapy v 4.8% control; five year benefit only about four per 1000 patients treated) and was not significant (2P=0.09).
Conclusions: Among a much wider range of patients at high risk of occlusive vascular disease than is currently treated routinely, some years of antiplatelet therapy - with aspirin 75-325 mg/day or some other antiplatelet regimen (provided there are no contraindications) - offers worthwhile protection against myocardial infarction, stroke, and death. Significant benefit is evident not only among patients with unstable angina, suspected acute myocardial infarction, or a past history of myocardial infarction, stroke, or transient ischaemic attack, but also among many other categories of high risk patients (such as those having vascular procedures and those with stable angina or peripheral vascular disease). There is as yet, however, no clear evidence on the balance of risks and benefits of antiplatelet therapy in primary prevention among low risk subjects.
Clinical implications
Clinical implications
Antiplatelet therapy protects a wider range of patients at high risk of occlusive vascular disease than is currently treated routinely: it should be considered for almost all with suspected acute myocardial infarction, unstable angina, or a history of myocardial infarction, angina, stroke, transient ischaemic attack, arterial bypass surgery, or angioplasty
There is, as yet, no clear evidence that antiplatelet therapy is indicated for routine use in “primary prevention” subjects at low risk of occlusive vascular events
Medium dose aspirin (75-325 mg/day) is the most widely tested antiplatelet regimen, and no other regimen appeared significantly more effective at preventing myocardial infarction, stroke, or death
Introduction
Previous Antiplatelet Trials And Aims Of Current Overview
It is reliably established that antiplatelet therapy reduces the risk of vascular death by about one sixth and the risk of non-fatal myocardial infarction and stroke by about one third in patients with unstable angina, suspected acute myocardial infarction, or a past history of myocardial infarction, stroke, or a transient ischaemic attack.*RF 1-4* There remains uncertainty, however, whether antiplatelet therapy is beneficial in other patient populations at high risk of occlusive vascular disease or in certain subgroups of these “high risk” populations (for example, among women or among patients who are old, hypertensive, or diabetic). It is also uncertain whether the benefits of long term antiplatelet therapy would outweigh the side effects among subjects in whom the risks of occlusive vascular disease are much lower (for example, primary prevention in the general population with no relevant medical history) and which antiplatelet regimens are most effective.
The aim of this second cycle of the worldwide Antiplatelet Trialists' Collaboration1 was therefore to assess the effects of antiplatelet therapy in more detail and in a much wider range of circumstances than before. This paper (part I in a series of three reports) describes the methods used in the collaborative overview process and then provides systematic overviews of the effects of “prolonged” antiplatelet therapy (that is, given for at least one month) in subjects at high risk and at low risk of occlusive vascular disease. The trials in high risk subjects are then subdivided more finely by the category of patients who were to be studied (prior myocardial infarction, acute myocardial infarction, prior stroke or transient ischaemic attack, and various other categories of patients considered to be at particular risk of vascular events because of their medical history). Where possible, the patients in those trials in high risk are also subdivided by certain personal characteristics (age, sex, blood pressure, diabetes) or by the type of antiplatelet regimen tested (aspirin at various doses, dipyridamole, ticlopidine, etc). In addition, the directly randomised comparisons of different antiplatelet regimens are reviewed. Randomised comparisons of different durations of treatment were not available, but the effects of antiplatelet therapy during year 1, during year 2, and during later times are examined separately to help assess any additional effects of more prolonged therapy.
Parts II and III will report overviews of 53 trials of antiplatelet therapy to maintain vessel patency after vascular procedures(super5) and 77 trials to prevent venous thromboembolism after general and orthopaedic surgery.6
Evidence That Can Be Generalised To A Wide Range Of Patients
Reliable detection (or refutation) of the sort of moderate sized benefits observed previously with antiplatelet therapy requires reliable exclusion both of moderate biases and of moderate random errors, either of which might obscure (or mimic) moderate treatment effects. Each requirement may be difficult to meet adequately without a proper overview of the unconfounded randomised trials, particularly if the aim is not only to distil clear findings from the overall material but also (by appropriate subgroup analyses) to help assess the generalisability of those findings.7 8
Analyses of the effects of treatment in particular subgroups will mainly involve “vascular events” (that is, non-fatal myocardial infarctions, non-fatal strokes, or vascular deaths) rather than vascular deaths alone. This is because such subgroup analyses may be statistically more reliable for vascular events (where, overall, there is a 13 standard deviation difference in favour of antiplatelet therapy; see results) than for vascular deaths alone (where there is “only” a six standard deviation difference in favour of antiplatelet therapy). Even for vascular events, however, separate analyses of the effects in an excessively large number of small subgroups of patients studied could well generate some false negative results merely by chance. Paradoxically, therefore, unless there are good reasons for expecting a difference in the direction of the effects of treatment in different settings the approximate benefit of antiplatelet therapy in some small subgroup of patients may best be assessed indirectly by approximate extrapolation from the proportional effect observed in a much wider class of patients.9
Materials and methods
Data Acquisition
Identification of all unconfounded randomised trials
The aim was to seek collaboration between the coordinators of all unconfounded randomised trials, published or unpublished,10 11 that could have been available for review by March 1990, in which antiplatelet therapy was compared with no antiplatelet therapy, or in which one antiplatelet regimen was compared with another (with the exception) of trials of antiplatelet therapy for patients with subarachnoid haemorrhage12 14 or for preventing pre-eclampsia15 or migraine16. Trials were to be included only if they were believed to have been randomised in a manner that precluded prior knowledge of the next treatment (for example, where allocation was not alternate or based on odd or even dates), and they were considered to be unconfounded if one treatment group differed from another only in the treatment of interest. Thus a trial in which antiplatelet therapy plus heparin was compared with the same heparin regimen would have been included whereas a trial of antiplatelet therapy plus heparin versus no treatment (or of antiplatelet therapy versus anticoagulant therapy) would not.
Relevant randomised trials were identified by computer aided literature searches (Medline and Current Contents), by manual searches of journals, by scrutiny of the reference lists of trial and review articles, by scrutiny of abstracts and meeting proceedings, by collaboration with the trials register of the International Committee on Thrombosis and Haemostasis, by inquiry among colleagues (particularly those who had coordinated other such studies), and by inquiry of various manufacturers of antiplatelet agents. This process and the correspondence with collaborating trialists that it engendered (see below) took several years. The aim was to include trials of agents whose primary mode of action on the vascular system was thought to be through inhibition of platelet aggregation or adhesion, or both: cyclo-oxygenase inhibitors (aspirin, flurbiprofen, ibuprofen, indobufen, naproxen, sulphinpyrazone, triflusal), phosphodiesterase inhibitors (dipyridamole, E5510, RA233), platelet calcium ion channel inhibitors (suloctidil), phospholipase inhibitors (hydroxychloroquine), thromboxane synthetase inhibitors, receptor blockers, or both (dazoxiben, piracetam, picotamide, ridogrel, sulotroban, daltroban, GR32191), and agents with direct effects on platelet membranes (ticlopidine). Agents known also to have a major vasodilating action (such as epoprostenol, oxpentifylline, ketanserin, naftidrofuryl) or major anticoagulant action (such as heparin or warfarin) were not to be included.
Definition of outcome measures
In this report the effects of antiplatelet therapy were to be assessed principally in terms of their effects on vascular events, defined as non-fatal myocardial infarctions, non-fatal strokes, or vascular deaths. Outcome events were to be counted as “non-fatal” only if the patient subsequently survived to the end of the study treatment period scheduled for that patient: otherwise, only the death was to be counted. Survivors could have suffered more than one type of non-fatal event. Causes of death were subdivided into “non-vascular” (that is, definitely non-vascular) and “vascular” (that is, definitely or possibly vascular, which includes all deaths attributed to cardiac, cerebral, haemorrhagic, embolic, other vascular, or unknown causes). Myocardial infarctions and strokes were to be counted if the investigator considered them to be either probable or definite. Transient ischaemic attacks (in brain or eye), angina, and “possible” myocardial infarctions or strokes were not to be counted as outcomes. Strokes (including subarachnoid haemorrhages) were to be counted only if symptoms persisted for at least 24 hours, and were subdivided into haemorrhagic (including those of “probably” haemorrhagic aetiology) and other (including those of probably ischaemic or of unknown aetiology). “Major” bleeds were those non-cerebral bleeds that required transfusion.
In trials among patients having vascular surgery or angioplasty or those having renal shunts or fistulas established, information on vessel or graft patency was sought (see part II5, and among all trials in which deep venous thromboses were looked for prospectively (usually among surgical patients) information on deep venous thromboses and pulmonary emboli was also sought (see part III6. Pulmonary emboli were to be counted if considered “probable” or “definite” by the investigator. There were differences between studies in the definitions of outcome measures, but because retrospective reclassification would have been impracticable (and potentially biased) the definitions preferred by the original investigators in each study were generally retained. The heterogeneity that this entailed does not invalidate the main overview results.17
“Summary data” from all contributing trials
For all studies that might have been randomised controlled trials of antiplatelet therapy a few simple details of trial design were requested from the principal investigators (including the exact method of treatment allocation, whether control patients received placebo, any other “blinding” of treatment allocation or outcome assessment, and the scheduled duration of trial treatment and of patient recruitment). Summary data were requested on the numbers of patients allocated to each treatment group and on the numbers of these who had suffered each of the outcomes of interest. These summary data were checked for internal consistency and for consistency with any published reports of the trials. When the data did not include information about outcome among all patients initially randomised or about all the outcomes of interest during the scheduled period of follow up, extra details were sought by correspondence with the principal investigators so that “intention to treat” analyses could be conducted. Before the final analyses, the data to be used were printed out for each trialist to check again.
Individual patient data from certain trial categories
For the trials among “low risk” subjects (that is, of primary prevention of vascular events) or among particular categories of “high risk” patients (those with unstable angina, acute myocardial infarction, prior myocardial infarction, stroke or transient ischaemic attack) data were sought for each individual randomised patient. These concerned certain baseline entry characteristics (age or date of birth, sex, blood pressure, and whether diabetic or not); the allocated treatments; and the dates of randomisation, of the scheduled end of trial treatment, of the actual end of treatment, of the last follow up, and of the first occurrence of any of the important vascular events defined above. More specific information about any non-vascular deaths and about the degree of disability associated with any strokes was also sought. In trials that recruited stroke or transient ischaemic attack patients information was sought on the nature of these qualifying cerebral events. The data from each investigator were checked for internal consistency of individual patient records, for balance of group sizes overall and according to certain prognostic categories, for consistency with the summary tabulations provided for each trial, and for some other indicators of possible anomalies.8 Queries were referred back for clarification, and the complete set of information on each trial was also referred back for confirmation.
Statistical Methods
Proportional and absolute reductions
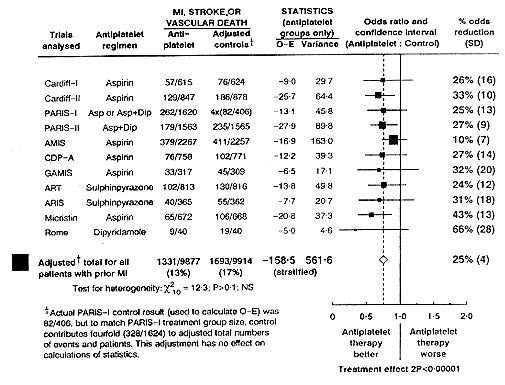
Both proportional and absolute reductions in clinical events can help in describing the size of any treatment effects. For example, overall in the 11 trials among patients with a history of myocardial infarction,*RF 18-40* 13% of the patients allocated antiplatelet therapy and 17% of the controls suffered a vascular event (myocardial infarction, stroke, or vascular death; fig 1). This absolute reduction of 4% (that is, about 40 vascular events prevented per 1000 patients treated) corresponds to a proportional reduction of about one quarter. Proportional reductions may be more widely generalisable to different medical circumstances, while absolute reductions may be more directly relevant to deciding whether to use treatment in particular medical circumstances. For these reasons both proportional and absolute reductions are described in the results.
Simplest summary of trial results: adjusted totals and adjusted percentages
Suppose that findings are to be combined from several trials that were all evenly randomised (that is, with about half the subjects in each trial allocated treatment and half control). A simple method of comparison would entail adding together all the treatment groups, adding together all the control groups, and, finally, comparing these two grand totals. If any of the trials had included deliberately uneven treatment allocation (for example, two thirds treatment, one third control), then it could first be adjusted to an evenly randomised comparison by counting the control group more than once. For example, in figure 1 for trials of antiplatelet therapy after myocardial infarction the small control group in the PARIS-I study(super22 23) would be counted fourfold to make it about the same size as the treatment group. The adjusted totals for the treatment and control groups would then be 262/1620 v 328/1624 in PARIS-I and 1331/9877 (13%) v 1693/9914 (17%) in all 11 trials together. In statistical principle these simple adjusted total may not be ideal (see below) but if, as here, the overall difference between treatment and control is very highly statistically significant, then such adjusted percentages (13% v 17%) may well provide a simple description of the effects of treatment that is sufficient for most practical medical purposes.
Comparisons of like versus like based on combination of “observed minus expected” differences in each separate trial
Figure 1 also illustrates the more formal statistical methods used to combine the results from different trials (using the actual numbers rather than adjusted numbers). These methods are completely robust, entailing no unjustified assumptions. A fuller description of the methods and of why they are more appropriate than other methods for such overviews of randomised trials is given elsewhere.17

Proportional effects on vascular events (myocardial infarction, stroke, or vascular death) in 11 randomised trials of prolonged antiplatelet therapy (for one month or more) versus control in patients with prior myocardial infarction. O-E=Observed minus expected Asp=Aspirin. Dip=Dipyridamole. MI=Myocardial infarction (In most trials patients were allocated roughly evenly between treatment groups, but in some (for example, PARIS-I) more were deliberately allocated to active treatment. To allow direct comparisons between percentages suffering an event in each treatment group, in figure 1 and elsewhere adjusted totals have been calculated after converting any unevenly randomised trials to even ones by counting control groups more than once. Statistical calculations are, however, based on actual numbers from individual trials. Ratio of odds of an event in treatment group to that in control group is plotted for each trial (black square: area proportional to amount of statistical information contributed by trial) along with its 99% confidence interval (horizontal line). All black squares are to left of solid vertical line, indicating benefit (but benefit is significant at 2P<0.01 only where, in three trials, entire confidence interval is to left of line). Stratified overview of results of all trials (and 95% confidence interval) is represented by open diamond, indicating odds ratio of 0.75 (SD 0.04) or, equivalently, odds reduction of 25% (SD 4%))
{kind=link}
Within each separate trial the standard quantity “observed minus expected” (together with its “variance”) is calculated for the numbers of events among treatment allocated patients.1 17 (Note that in an evenly randomised trial the observed minus expected value equals only half the number of events that appear to have been avoided by treatment.) To combine information from several different trials these observed minus expected values - one from each trial - can simply be added up. If treatment did nothing, then each of the separate observed minus expected values could equally well be positive or negative and their grand total would likewise differ only randomly from zero. On the other hand, if treatment reduced the risk of adverse outcome to some extent in most or all of the trials, then any individual observed minus expected value would be likely to be somewhat negative (that is, favouring treatment), so that when all these values are added up their grand total may be clearly negative. (These arguments do not assume that the size of the treatment effect is the same in all patients, or in all trials; indeed, it probably is not.) So, for example, in figure 1 the grand total of the individual observed minus expected values is -158.5. The negative sign indicates fewer vascular events in the patients allocated antiplatelet therapy than in the controls, and the numerical value of -158.5 suggests (very approximately) that about 320 vascular events were averted by treatment.
Variances and P values
The variance of the observed minus expected value is small in small trials and large in large, informative trials that estimate more accurately the proportional reduction in adverse events. Indeed, the variance of the observed minus expected value indicates the “statistical information content” of a trial.17 For the grand total of several observed minus expected values, the variance is given simply by the sum of their individual variances, and the standard deviation is the square root of this sum. In figure 1 the grand total of -158.5 has a variance of 561.6 and hence a standard deviation of 23.7, so it differs from zero by nearly seven of its standard deviations. This indicates a highly significant protective effect of antiplatelet therapy (two sided P value (2P) <0.00001), as a difference of only two standard deviations would have been enough for conventional statistical significance (2P<0.05). P values >=0.1 are denoted non-significant (NS).
Proportional odds reductions
The grand totals (G and V) of the individual observed minus expected values and of their variances can be used not only (as above) to calculate a P value to help test whether treatment has any effect but also to help describe the size of the treatment effect. This description entails calculating (by using the formula exp(G/V)) the “typical odds ratio,” which gives the ratio of the odds of an unfavourable outcome among treatment allocated patients to the corresponding odd among controls, stratified by trial. In figure 1 allocation to antiplatelet therapy is associated with a typical odd ratio of 0.75, which corresponds to a reduction of 25% in the odds of a vascular event.
Proportional odds and risk reductions
When comparing outcome among treated and control patients in trial analyses where substantial proportions have not yet suffered the outcome of interest, “odds” reductions and “risk” reductions are not importantly different from each other as method: for describing the results. For example, if 100 control patients suffered a vascular event and 500 did not, then the odds of suffering an event would be one to five, or 0.20, while the risk would be one in six. In this instance it can be shown that a 25% odds reduction (from 0.20 to 0.15) would correspond to a 22% risk reduction (from 100/600 to 78/600). The percentage reduction in odds will always be slightly larger, but the similarity of these reductions (25% and 22%) confirms that it does not matter which is used to describe the trial results. Odds ratios for overviews are simpler to calculate, and so use is chiefly made of percentage reductions in odds in this report.
Standard deviations and confidence intervals
A convenient way of describing the statistical reliability of an odds reduction is to give its standard deviation (SD). For example, the overall odds reduction in figure 1 is given as 25% (SD 4%). Two standard deviations below and above 25% would yield 17% (one sixth) and 33% (one third), indicating that unless a rather unlikely (2P<0.05) chance event has occurred the odds reduction lies somewhere in the range between one sixth and one third. A more precisely calculated version of this “95% confidence interval” (with ends at exp(G/V +/- 1.96/V) is denoted by an open diamond in figure 1 and subsequent figures. The odds ratio observed in each of the parts that contribute to the total is plotted as a black square, with the areas of the squares chosen to be approximately proportional to the numbers of events (that is, the “statistical information content”) in each trial. The horizontal line through each black square indicates the 99% confidence interval for the odds ratio - that is, the range of odds ratios with which that result is reasonably comfortably compatible. Because, appropriately,17 assumption free (that is, “fixed effect”) statistical methods are used to combine trial results the standard deviations and confidence intervals describe the extent to which the play of chance during the randomisation process would be apt to affect the results, either of one particular trial or of an overview of several trials.
FIG 3 - Absolute effects of antiplatelet therapy (145 trials) on vascular events (myocardial infarction, stroke, or vascular death) in four main high risk categories of trial and in low risk (primary prevention) (Adjusted totals calculated after converting any unevenly randomised trials to even ones by counting control groups more than once, for calculating adjusted percentages and events prevented per 1000 patients allocated antiplatelet therapy. Statistical significance (2P) based on stratified analyses of original, unadjusted numbers in each trial (see statistical methods))

(Dagger)Months of A=Means of scheduled antiplatelet durations. No trial lasted under one month.
{kind=link}
Description Of Trials
A total of 413 apparently randomised trials of antiplatelet therapy could have been identified by March 1990.*RF 18-20* On further investigation 49 were not properly randomised,*RF 313-363* 51 were confounded or had extremely large numbers of subjects lost to follow up or included a crossover design*RF 364-420* (plus A Lowenthal, personal communication), and two (Birmingham ticlopidine study and PACT) had never started. Data from one study (Zurich vein bypass study) were not available owing to the death of the investigator (A Bollinger, personal communication). Results from 53 studies, many of which were still in progress, were not available in March 1990*RF 276-313* and, although results from some are now available (and, for the larger

Proportional effects of antiplatelet therapy (145 trials) on vascular events (myocardial infarction, stroke, or vascular death) in four main high risk categories of trial and in low risk (primary prevention). TIA = Transient ischaemic attack (Stratified ratio of odds of an event in treatment groups to that in control groups is plotted for each group of trials (black square) along with its 99% confidence interval (horizontal line). Overviews of results for certain subtotals (and 95% confidence intervals) are represented by diamonds. Odds reduction observed in particular groups of trials are given to right of solid vertical line) trials, are included in the appendices and discussion), they do not contribute to the main analyses. This left 257 eligible trials among 118 958 patients. Trials of less than one month of antiplatelet therapy were not to be included in the analyses in this report. They were, with few exceptions*RF 249-275* (see appendices 1 and 2), mostly designed to assess efficacy in terms of vessel or graft patency (see part II5 or in terms of the prevention of deep venous thrombosis or pulmonary embolism after surgery (see part III6.
{kind=link}

Proportional effects of antiplatelet therapy (145 trials) on non-fatal myocardial infarction, non-fatal stroke, vascular death, and any death in four main high risk categories of trial and in low risk (primary prevention). Symbols and conventions as in figures 1 and 2
{kind=link}
Appendices 1 and 2 give details of the 159 randomised trials of prolonged (that is, one month or more) antiplatelet therapy versus control among 96 935 patients (with individual patient data for 32 of these trials among 73 933 patients) and of the 32 trials comparing different prolonged antiplatelet regimens among 13 655 patients (with some patients in 16 of these trials also contributing to the comparison of antiplatelet versus control).*RF 18-248* For some trials the results differ from those originally published, generally because of the considerable efforts taken to obtain complete follow up data on all randomised subjects (see above), including not only events while treatment actually continued but also events before the scheduled end of trial treatment (which was on a common date for all patients in some trials and at a fixed interval after randomisation in others).
Results
Effects Of Antiplatelet Therapy On “Vascular Events”
Information about vascular events (non-fatal myocardial infarction, non-fatal stroke, or vascular death) was available from 145 trials among a total of 51 144 patients allocated antiplatelet therapy and 45 172 controls (adjusted control total 51 315; fig 2) and was known to be unavailable from 14 small trials among a total of only 619 patients. The total numbers of patients suffering a vascular event among those allocated antiplatelet therapy were 4835 (9.5%) of 51 144, while the corresponding adjusted total among the controls was 6108 of 51 315 (11.9%). In the formal statistical analysis the grand total of observed minus expected values was about - 600, indicating that about 1200 vascular events were prevented. Overall in these trials the typical reduction in the odds of suffering such events was 25% (SD 2%), which was very highly significantly favourable (13.1 standard deviations from zero; 2P<0.00001) (fig 2).
Although the 145 trials did not all indicate exactly the same odds reduction, the amount of scatter between their separate results was no greater than might be expected by chance if the true odds reduction in each study was exactly 25%. But when the trials were subdivided into five main categories, the proportional reductions seemed to be somewhat greater in the four “high risk” categories than in the one “low risk category” (P=0.001 for this heterogeneity; fig 2). The proportional reductions in vascular events were each about one quarter and highly significant (2P<0.00001) in each of the four high risk categories - namely, patients with a prior history of myocardial infarction, patients with suspected or definite acute myocardial infarction, patients with a prior history of stroke or transient ischaemic attack, and patients with other evidence of vascular disease or some condition associated with an increased risk of occlusive disease.
Effects of antiplatelet therapy on fatal and non-fatal strokes, aetiology
As the proportional reductions were bigger among the high risk patients, the absolute risk reductions were very much bigger (ranging from 23 to 38 vascular events averted per 1000 high risk patients allocated antiplatelet therapy; fig 3) than among the low risk “primary prevention” subjects studied. For the latter group, the proportional reduction was less extreme (10% (SD 6%) and the absolute risk in the control group was low (only 4.8% of controls suffered an event during about five years of follow up; fig 3). Hence the absolute benefit of antiplatelet therapy seemed small (only about four vascular events averted for every 1000 patients treated for five years), and even this small benefit among such low risk subjects was statistically uncertain (2P=0.09).
Effects On Different Measures Of Outcome
Myocardial infarction
The information on non-fatal myocardial infarction was only about 95% complete, but the reductions in non-fatal myocardial infarction were so significantly and substantially different from zero that the unavailability of some data is unlikely to be important. Non-fatal myocardial infarctions were recorded in 122 trials, and the typical odds reduction produced by allocation to active treatment was 34% (SD 3%) (2P<0.00001; fig 4). This reduction in non-fatal myocardial infarction was highly statistically significant, not only in each of the four high risk categories but also in the low risk category, which suggests that a similar proportional reduction in myocardial infarction can be expected in a very wide range of settings.
Stroke
For non-fatal stroke, the information was also about 95% complete (124 trials provided results) and the typical odds reduction observed overall was large (25% (SD 4%)) and highly significant (2P<0.00001; fig 4). The reduction in non-fatal stroke among high risk patients was very definite (31% (SD 5%)) and about the same size as the reduction in myocardial infarction. There was no significant heterogeneity between the proportional odds reductions in stroke in the four high risk categories (fig 4), but the effects were very different in high risk and low risk subjects (P=0.00002 for heterogeneity). Indeed, in the low risk primary prevention studies the effect of antiplatelet therapy on non-fatal stroke appeared unfavourable. This unfavourable result was, however, statistically uncertain, and the true effect on stroke in such low risk subjects might still be about zero.
In addition to the 2000 non-fatal strokes recorded, about 500 fatal strokes were recorded during the scheduled treatment periods. Subdivision of all strokes, fatal or not, with respect to what is known of their aetiology (table) indicated that a probable small increase in haemorrhagic strokes was outweighed by a larger and very definite reduction in other strokes. The table shows that haemorrhage was considered to be the probable or definite aetiology of about 25% of fatal strokes but only about 5% of non-fatal strokes. This may help explain why the apparent effect on fatal strokes (15% (SD 9%) reduction; NS) was non-significantly smaller than the effect on non-fatal strokes (25% (SD 4%) reduction; 2P<0.00001).
Reliable analyses of disabling and other non-fatal strokes were not separately available because in only 15 trials (14 high risk, one low risk227 could non-fatal strokes be divided into those that were “disabling” (that is, severe interference to daily life persisting for some months after the stroke occurred) and those that were not. In these 14 high risk trials, antiplatelet therapy was associated with a 24% (SD 9%) reduction (2P<0.01) in disabling or fatal stroke and a 17% (SD 10%) reduction (2P=0.09) in non-disabling stroke with subsequent survival, the standard deviations of both reductions being large.
Vascular deaths
All but one of the 145 trials provided information on mortality, most deaths being attributed to vascular causes (which, by definition, include unknown causes). The overall effect of antiplatelet therapy on such “vascular” deaths was highly significantly favourable (6.7 standard deviations from zero; 2P<0.00001), and the typical reduction in the odds of vascular death was 17% (SD 3%). Similar proportional reductions were observed in the four high risk categories, but little net effect on vascular death was observed in the primary prevention trials, and the difference between the definite mortality reduction in the high risk categories and the lack of apparent effect in the low risk primary prevention trials approached significance (P=0.07; fig 4).
Non-vascular and total deaths
There was also a slight but non-significant tendency for there to be fewer non-vascular deaths among patients allocated antiplatelet therapy than among controls (figs 4, 5). Consequently, total (all cause) mortality was significantly (1P<0.01) reduced in each high risk category of patients but not in low risk subjects (fig 4). If antiplatelet therapy has some unanticipated protective or adverse effect on some specific type of non-vascular death, a crude overall analysis of non-vascular mortality might well yield an uninformatively non-significant result. Fatal non-cerebral bleeding was recorded only rarely (11/51069 (0.02%) patients among those allocated antiplatelet therapy versus 18/51 246 (0.04%) adjusted controls; NS) but there was a significant excess of three per 1000 “major” non-fatal non-cerebral bleeds (214/37 772 (0.6%) v 116/37 817 (0.3%); 2P<0.00001).

Absolute effects of antiplatelet therapy on various outcomes in 11 trials in patients with prior (but not acute) myocardial infarction, five trials in patients with acute myocardial infarction (suspected or definite), 17 trials in patients with prior stroke or transient ischaemic attack, and three trials in people at low risk (primary prevention). Conventions as in figure 3. In “any death” columns non-vascular deaths are represented by lower horizontal lines (and may be calculated by subtracting vascular deaths from any deaths)
{kind=link}
In all but one228,229 of the 32 trials for which individual patient data were obtained more specific details about the causes of other non-vascular deaths were available. Separate analysis of those trials also indicated a non-significant shortfall in all non-vascular deaths (352 observed, 378.2 expected) among antiplatelet allocated patients that was similar to that seen overall (679 observed, 699.3 expected; fig 4), with slightly, though non-significantly, fewer deaths both from cancer (183 observed, 196.6 expected) and from other non-vascular causes (169 observed, 181.6 expected). Site specific data on cancer deaths were not available, so the suggestion that aspirin might prevent intestinal cancer421 or that it might cause renal cancer422 could not be addressed directly (although analyses of one of the longest of the randomised trials of aspirin did not find any evidence of an excess of renal cancer423.
Effects In Different Categories Of Patients Patients with history of myocardial infarction
The weighted (by study size) mean duration of antiplatelet therapy in trials among about 20 000 patients with a prior history of myocardial infarction was 27 months, and allocation to antiplatelet therapy produced a highly significant reduction (2P<0.00001) of about 36 per 1000 in the risk of suffering another vascular event (fig 3). The standard deviation of this risk reduction was only 6, so the real risk reduction was unlikely to be less than about 20 or 30 per 1000. Moreover, here, as in other statistically definite trial results, the benefits of actually taking treatment tend to be underestimated by clinical trials because some patients did not comply fully with their random allocation (see discussion). Among patients with a prior history of myocardial infarction there were large and highly significant reductions in non-fatal reinfarction (18 (SD 4) prevented per 1000; 2P<0.00001; (fig 5)) and in vascular death (13 (SD 5) per 1000; P<0.005: total mortality also significantly reduced) and a smaller but still highly significant reduction in non-fatal stroke (6 (SD 2) per 1000; 2P=0.0005).
Patients with suspected or definite acute myocardial infarction
For acute myocardial infarction the overview was again based on almost 20 000 patients, nearly all of whom were in the ISIS-2 trial of one month of 160 mg aspirin daily in suspected acute myocardial infarction.43 Allocation to antiplatelet therapy produced a highly significant reduction (2P<0.00001) of 38 per 1000 in the risk of suffering a subsequent vascular event (fig 3), again with a fairly small standard deviation. Most of this reduction was in vascular deaths (24 (SD 4) prevented per 1000; 2P<0.00001 (fig 5)), but there was also a highly significant reduction in non-fatal reinfarction during the month of treatment (12 (SD 2) per 1000; 2P<0.00001) and a smaller but still significant reduction in non-fatal stroke (2 (SD 1) per 1000; 2P<0.02).
Patients with history of stroke or transient ischaemic attack
Among more than 10 000 patients with a prior history of stroke or transient ischaemic attack, allocation to a mean duration of 33 months of antiplatelet therapy produced a highly significant (2P<0.00001) reduction of 37 per 1000 in the risk of suffering another vascular event (fig 3), with a standard deviation of 8. Compared with patients after a myocardial infarction, patients after a stroke or transient ischaemic attack are at relatively high absolute risk of stroke recurrence and at relatively low absolute risk of non-fatal myocardial infarction. Among such patients, therefore, there was a large and highly significant absolute reduction in non-fatal stroke (20 (SD 6) prevented per 1000; 2P<0.0005 (fig 5)) plus a somewhat smaller but still highly significant reduction in non-fatal myocardial infarction (9 (SD 3) per 1000; 2P=0.001). Although the reduction of 11 (SD 6) per 1000 vascular deaths was only marginally significant (2P<0.05) on its own, the highly significant reductions in non-fatal vascular events and the significant (2P<0.01) reduction in all cause mortality strongly reinforce the conclusion that prolonged antiplatelet therapy reduces both the vascular and all cause mortality in patients with a history of stroke or transient ischaemic attack.
For 10 of the 12 such trials that provided individual patient data it was possible to categorise patients into those who had presented with completed stroke and those who had presented with transient ischaemic attack only. The proportional reduction in important vascular events in these cerebrovascular trials was 22% (SD 5%) overall and was similar for patients presenting with a completed stroke (23% (SD 7%) reduction; 2P<0.001) and for those presenting with only a transient ischaemic attack (22% (SD 7%) reduction; 2P<0.01).
Low risk “primary prevention” subjects
Among about 28 000 low risk “primary prevention” subjects studied, allocation to an average of just over five years of antiplatelet therapy produced a small but highly significant (2P<0.0005) reduction of 5 (SD 2) per 1000 in non-fatal myocardial infarction (fig 5), but the reduction in vascular events was slightly smaller and less clearly significant (figs 2, 3; 2P=0.09). In contrast with the highly significant reduction in non-fatal strokes among high risk subjects there was no evidence of any decrease in non-fatal strokes among these low risk subjects - rather the reverse (2 (SD 1) per 1000 increase; NS).
When the aetiology of all strokes (fatal and not; table) observed among low risk subjects was considered there was not only a small, marginally significant (2P<0.05) excess of strokes attributed to haemorrhagic causes but also a non-significant excess of “other” strokes. This may be because other strokes included those of unknown cause, a few of which may have been haemorrhagic and caused by antiplatelet therapy. But as a large proportion of these other strokes were confirmed as occlusive, the adverse effects on stroke among these low risk subjects may well have been inflated to some extent by chance. Haemorrhagic strokes are more likely to be fatal, and a small excess of these with antiplatelet therapy among the low risk primary prevention subjects may account, at least in part, for the lack of any significant difference in vascular mortality (table, fig 5).
Other high risk patients
The remaining 20 000 high risk patients represented a mixed category of conditions associated with an increased risk of vascular events. Among them, the mean duration of antiplatelet therapy was only about half as long as in the post-myocardial infarction or post-stroke or transient ischaemic attack trials. Hence, although the event rates per month (and the benefits of antiplatelet therapy per month; see below) were about as large as in those trials, the cumulative rates of vascular events (and hence the cumulative benefits of antiplatelet therapy) were only about half as great. The benefits were, however, statistically definite (2P<0.00001; fig 3); allocation to an average of 16 months of antiplatelet therapy in these other high risk patients producing a reduction of 23 per 1000 in the risk of suffering a vascular event, again with a small standard deviation (SD 4). Among these patients there were separately significant reductions in non-fatal myocardial infarction, non-fatal stroke, vascular death, and total mortality (fig 4).
Figure 6 subdivides this fourth large category of high risk patients into 14 subcategories, comparing their results with each other and with the first three large categories (prior myocardial infarction, acute myocardial infarction, prior stroke or transient ischaemic attack). Patients in each of these three large categories and 14 small subcategories were, for one reason or another, at high risk of occlusive vascular disease. Thus in view of the overall results for high risk patients (odds reduction 27% (SD 2%)) some protection might be expected from antiplatelet therapy for each subcategory. But if there were a real benefit that was of roughly similar size in each subcategory, then what was likely to be observed was significant benefit in a few, non-significant benefit in most, and no particularly striking evidence of heterogeneity around the overall odds reduction of about a quarter (indicated by the vertical broken line in figure 6).
This is exactly what is shown in figure 6. Although almost all of the subcategory results appear to favour treatment, the reductions are conventionally significant at 2P<0.01 (as indicated by the 99% confidence intervals not crossing the solid vertical line) only for patients with unstable angina (182 v 285 events; 2P<0.00001), for those who had undergone percutaneous transluminal coronary angioplasty (32 v 61 events; 2P=0.002), and for those who had undergone heart valve surgery (46 v 79 events; 2P<0.01) and not for the other 11 subcategories. But there was no significant evidence of heterogeneity between the

Proportional effects of antiplatelet therapy on vascular events in 142 trials in high risk patients subdivided by type of trial. Symbols and conventions as in figures 1 and 2. CABG=Coronary artery bypass grafting. PTCA=Percutaneous transluminal coronary angioplasty. CAD=Coronary artery disease
{kind=link}
results in figure 6, and the most appropriate conclusion may well be that antiplatelet therapy is likely to be protective for any high risk patients with clinically evident occlusive vascular disease, unless there is some special contraindication (see discussion, which includes those major trials that became available only after March 1990).
Subdivision by other characteristics in high risk patients
In those trials in high risk patients where data for each subject were available, treatment produced similar proportional reductions in middle age and old age, in men and women, in hypertensive and normotensive patients, and in diabetic and non-diabetic patients (fig 7). None of these characteristics are therefore contraindications to antiplatelet therapy for patients who have occlusive vascular disease. In particular, women seem to derive about as much benefit as men, and elderly patients seem in the short term to derive even more benefit than middle aged patients might do (although, as middle aged patients have a long life expectancy, their long term benefit may be greater).

Absolute effects of antiplatelet therapy on vascular events in the 29 trials in high risk patients with separate information available on each patient subdivided by age and sex and by diastolic blood pressure and diabetes. Conventions as in 3
{kind=link}
Comparisons Of Different Antiplatelet Regimens Direct comparisons between different regimens
Any real differences between two antiplatelet regimens are likely to be smaller than the differences between antiplatelet and no antiplatelet treatment. Hence tens of thousands of patients may need to be randomised directly between different antiplatelet regimens to ensure (by large numbers) small enough random errors and to avoid (by direct randomisation) important biases. Unfortunately, the numbers so far randomised between one antiplatelet regimen and another have been much smaller than this.
8 gives the four comparisons, where, in aggregate, at least 1000 patients were randomised, though the largest included only a few thousand patients. There was no significant difference between the protective effects of higher aspirin doses (500-1500 mg daily) and of medium aspirin doses (75-325 mg daily), but these direct randomised comparisons were based on only 396 vascular events in three trials. So, although these comparisons of different aspirin doses do not show any need for more than 300 or 325 mg daily (and a dose much higher than this would be significantly more gastrotoxic69,70, they cannot prove that no worthwhile differences exist (for example, of 10% or 20% in either direction). Similarly, in the direct comparisons of aspirin alone versus aspirin plus dipyridamole, of aspirin versus sulphinpyrazone, or of aspirin versus ticlopidine the differences in the combined outcome measure of vascular events were not statistically significant (though moderate differences cannot be ruled out).

Direct comparisons of proportional effects on vascular events of different antiplatelet regimens in trials in over 1000 high risk patients. Symbols and conventions as in figures 1 and 2
{kind=link}
Indirect comparisons between different regimens
The effects of different regimens can also be compared indirectly by comparing the size of the protective effect observed in the trials of one particular antiplatelet regimen versus control with the size of the protective effect in trials of another antiplatelet regimen versus control. Such indirect comparisons need to be interpreted more cautiously, for although many of the biases inherent in non-random methods (such as those involving historical controls) are avoided, some potential for bias remains.17 This potential may, however, be reduced by restricting attention to the 142 trials of antiplatelet therapy versus control in high risk patients and by comparing proportional rather than absolute risk reductions. When this was done (fig 9) the effects of the different antiplatelet drug regimens that have been tested in these trials appeared remarkably homogeneous. None of these groups of antiplatelet regimens appeared to be much more or less effective than any other, irrespective of whether they were characterised just by the drugs they contain or, for aspirin, by the daily dosage. (The formal statistical comparisons confirm that there was no significant heterogeneity between the protective effects of the seven different drug combinations in figure 9.)

Indirect comparisons of proportional effects on vascular events of different antiplatelet regimens in 142 trials in high risk patients. Symbols and conventions as in figures 1 and 2. Sulph = Sulphinpyrazone
{kind=link}
Aspirin regimens were much the most widely tested in such trials, accounting for two thirds of the data in figure 9. Overall, aspirin was associated with a highly significant 25% (SD 2%) proportional reduction (2P<0.00001) in vascular events, with at least as great an apparent effect in trials of medium daily doses of 75-325 mg daily (less than 160 mg daily (mostly 75-150 mg), 26% (SD 11%) reduction (2P=0.01); 160-325 mg daily, 28% (SD 3%) reduction (2P<0.00001) as in trials of higher doses (500-1500 mg daily, 21% (SD 4%) reduction (2P<0.00001)). These aspirin trials, together with two more recent studies of 75 mg/day(super 277 279) (see discussion), provide substantial evidence that in emergency use (for example, in acute myocardial infarction(super43) doses as low as 160 mg are effective and that in long term use doses as low as 75 mg daily are effective; however, they provide no substantial evidence about daily doses of less than 75 mg.
The numbers studied in trials of the six other antiplatelet drug combinations were smaller, so that estimates of the sizes of the protective effects were less accurate than for aspirin alone. For three combinations (aspirin plus sulphinpyrazone, dipyridamole alone, and suloctidil alone) the numbers studied were so small that although the apparent effects were about as great as for aspirin, the confidence intervals included zero. For the three other drug regimens (aspirin plus dipyridamole, sulphinpyrazone alone, and ticlopidine alone) the numbers studied were larger and the protective effects were significantly different from zero; they were not, however, significantly different from each other or from the size of the reduction that can be produced by aspirin alone.
Duration Of Antiplatelet Treatment
No large randomised trials have compared different durations of antiplatelet treatment. Some information may be gained by determining whether in trials where treatment was prolonged the absolute benefits of treatment continued to grow with time. But such comparisons would eventually become somewhat biased against an effective treatment (see discussion). Hence whatever further divergence there may be between treatment and control in later years tends to underestimate the benefits that would be seen in an appropriately randomised comparison between stopping and continuing treatment.
For the trials of more than one year of antiplatelet therapy among patients with prior myocardial infarction, stroke, or transient ischaemic attack in which information was available on the times of each individual event, figure 10 shows the apparent effects of treatment in each separate year. The largest amounts of data, and the largest benefit, were seen in the first year, but the further benefit just during year 2 was highly significant (the odds reduction during that year alone was 24% (SD 5%); 2P<0.0001), and even after year 2 there appeared to be some additional benefit (if non-significant). These year by year risk reductions are plotted17 in figure 11, which shows that the absolute benefit among such high-risk patients was already substantial by the end of the first year, that it grew significantly larger by the end of year 3, and that there was no evidence that treatment stopped being protective. Figure 11 also shows substantial benefits at the end of only one month of treatment in patients with acute myocardial infarction (2P<0.00001) and at the end of six months of treatment in patients with unstable angina (2P<0.00001), but in primary prevention the absolute annual benefit even after five years was still small and not conventionally significant (2P = 0.08).

Proportional effects on vascular events in trials among patients with prior myocardial infarction, stroke, or transient ischaemic attack showing additional benefits during different time periods of antiplatelet therapy. (Twenty one trials with more than one year of treatment and separate information on each patient.) Symbols and conventions as in figures 1 and 2. In the three primary prevention trials, comparable stratified observed minus expected and variance statistics were minus 12.5 and 51.3 (year 1); minus 7.2 and 56.1 (year 2); minus 3.5 and 50.3 (year 3); minus 12.2 and 51.4 (year 4); and 0.3 and 70.4 (year 5)
{kind=link}

Years to first vascular event after randomisation (stroke, myocardial infarction, or vascular death) in the 32 trials of antiplatelet therapy with separate information on each patient (Adaptation of standard life table method permitting unbiased combination of information from heterogeneous trials17 was used to plot year by year results from figure 10 for high risk patients with previous myocardial infarction, stroke, or transient ischaemic attack and for primary prevention among low risk subjects. Median treatment duration was used to plot overall results from figure 6 for trials in acute myocardial infarction (one month) and in unstable angina (six months))
{kind=link}
Discussion
Benefit In a Wide Range Of Patients At High Risk Of Occlusive Vascular Disease
These results strongly reinforce and extend the results of the first cycle of the Antiplatelet Trialists' Collaboration.1 Antiplatelet therapy has been shown to reduce the risk of “vascular events” (non-fatal myocardial infarction, non-fatal stroke, or vascular death) by about one quarter, not just among patients with unstable angina, acute myocardial infarction, or a past history of myocardial infarction, stroke, or transient ischaemic attack but also in the large category of other patients at increased risk of occlusive vascular disease (that is, patients having coronary vascular procedures and patients with stable angina, valvular heart disease, atrial fibrillation, or peripheral vascular disease). Vascular mortality and all cause mortality were also significantly reduced by antiplatelet therapy in these high risk patients, and compared with these benefits the absolute risk of fatal and major non-fatal bleeds was small.424
Because these proportional risk reductions were statistically reliable and appeared approximately homogeneous over the wide range of settings studied in these trials, protective effects of antiplatelet therapy against occlusive vascular disease should be expected for a range of high risk patients that is even wider than just those categories in which this overview provides direct evidence of benefit. This important conclusion depends partly on the definiteness and consistency of the evidence of benefit in all categories of high risk patients that have been studied extensively (fig 2) and partly on the common sense notion that if antiplatelet therapy averts a certain proportion of occlusive vascular events in one category of patients, then although the proportion averted in another category may not be identical it is unlikely to be vastly different - and, in particular, is extremely unlikely to be zero. (The mathematical theory of James-Stein estimators 9 provides formal statistical support for this emphasis on the overall results.) It would therefore be inappropriate to draw conclusions about each small subcategory that are based only on the results from that subcategory.
Compare, for example, the apparently contrasting effects in figure 6 of antiplatelet therapy on vascular events in the trials among patients with coronary artery disease who had undergone percutaneous transluminal coronary angioplasty (32/663 v 61/669, an apparent halving of risk that was highly significantly different from zero) and among those who had undergone coronary artery bypass grafting (124/2529 v 127/2546, showing no apparent difference from zero). It is not reasonable to suppose that antiplatelet therapy halves vascular events during the months after angioplasty but has no effect on them in the months after bypass surgery, especially as we know (part II5) that some months of antiplatelet therapy after bypass surgery produces a massively significant reduction in the likelihood (measured angiographically) of the bypass becoming occluded.
Consequently, even though this overview of existing data does not provide direct evidence of benefit among certain categories of patient at high risk of occlusive vascular disease that have not been extensively studied, it provides indirect evidence that the net effects would be beneficial, unless there is some particular reason to expect serious side effects. It is possible to extrapolate too far and so reach mistaken conclusions that lead to inappropriate treatment, but it is also possible that taking too formal a view of the existing evidence and not extrapolating far enough may lead to inappropriately restrictive treatment policies that deny antiplatelet therapy to many patients who would benefit. Thus the information from trials in this overview may provide useful guidance in the treatment of a far wider range of high risk patients than just those studied, although the further the extrapolation the more desirable it might be to have direct evidence.
In particular, directly randomised evidence will certainly be needed in those conditions (such as acute stroke) where there are special risks of bleeding with antiplatelet therapy that might outweigh the reduction in occlusive disease (and for acute stroke this is currently being sought in the international stroke trial425).
In other circumstances, however, it would be reasonable to infer that, provided there was no definite contraindication, antiplatelet therapy would probably be of net benefit for all categories of patients who are currently at high risk of occlusive vascular disease. Support for this conclusion is provided by studies reported after March 1990. For example, this overview included only about 600 patients with stable angina and did not on its own show clearly for such patients that antiplatelet therapy reduced the risk of vascular events. But after adding the recently reported results for vascular events from the SAPAT study in stable angina279 (111/1009 aspirin v 159/1026 placebo; appendix 1) and the United States Physicians' health study426 of patients who had stable angina at entry (24/178 aspirin v 25/155 placebo) there was a highly significant 33% (SD 9%) benefit (2P<0.0005) among the new total of 3000 patients with stable angina, which was similar to the benefit in other high risk patient categories.
In contrast, for people whose absolute rates of ischaemic events are low (for example, “primary prevention” among apparently healthy people) or for people who are at particularly high risk of a major haemorrhagic event (for example, those with a recent history of possible cerebral haemorrhage) even a small increase in serious haemorrhagic events might outweigh the expected decrease in ischaemic events. For example, in the low risk primary prevention studies conducted so far, the non-significant reduction in vascular events (2P=0.09;fig3) combines a definite reduction in non-fatal myocardial infarction (29% (SD 8%) decrease; 2P<0.0005), a possible increase in non-fatal stroke (21% (SD 13%) increase; NS), and no apparent effect on vascular mortality (2% (SD 10%) reduction). Because of this uncertainty and because the numbers to whom this could be relevant are so large, more directly randomised evidence is needed on whether long term prophylactic antiplatelet therapy produces any worthwhile net benefit in “primary” prevention, both among subjects with raised levels of coronary risk factors (hypercholesterolaemia, hypertension, renal disease, etc) and among those without. Both are being sought (for example, in the thrombosis prevention trial,309 the planned British Hypertension Society study, and the United States Women's Health study427.
Benefit Irrespective Of Age, Sex, Blood Pressure, And Diabetes
In those studies of high risk subjects in which individual patient data were obtained, separate analyses were planned among older (aged 65 or over) and younger patients, among women and men, among hypertensive (diastolic blood pressure 90 mm Hg or over) and “normotensive” patients, and among diabetic and non-diabetic patients. In each case antiplatelet therapy for high risk patients appeared to reduce the odds of vascular events by a roughly similar proportion (fig 7). Thus the notion that women might not benefit from antiplatelet therapy (which arose from data dependent subgroup analyses of a few trials*RF 57-59* is contradicted by these much more reliable, prospectively planned overview analyses. Older patients, patients with hypertension, and diabetics tend to be at higher than average risk of vascular events, and if the proportional benefit is similar, then the absolute benefits of antiplatelet therapy may be greater than average among them (fig 7), certainly in the first few years of treatment. (Additional evidence among diabetic patients has recently been provided by the large ETDRS trial of five years of aspirin282; no special hazards of antiplatelet therapy for diabetics were seen283 and vascular events appeared to be reduced, though not significantly (350/1856 v 379/1855 (NS); appendix 1).)
Lack Of Evidence Of Differences Between Different Antiplatelet Regimens
Most of the trials tested aspirin, although a substantial minority tested other drugs. Two main questions may therefore be addressed. Firstly, if aspirin is to be used as the only drug, which range of doses seems most promising? Secondly, is some other antiplatelet drug or combination of drugs better than aspirin alone?
Aspirin pharmacology
Within a few days of beginning treatment with at least 75 mg aspirin daily the enzyme cyclo-oxygenase is virtually completely inhibited, both in platelets (producing an antithrombotic effect) and in arterial walls (which may possibly produce some impairment of the antithrombotic effect by reducing prostacyclin production in the vascular endothelium, although the relevance of this is disputed).*RF 428-431* It is not known whether doses somewhat lower than this have a greater or lesser therapeutic effect. At 75 mg or more daily, however, across the 20-fold range of doses up to 1500 mg/day that have been studied widely in the trials in this overview, the pharmacological evidence on cyclooxygenase gives no reason to expect any material difference either on platelets or on vessel walls between different daily doses. Nevertheless, to achieve virtually complete inhibition immediately, aspirin treatment in emergency situations such as acute myocardial infarction, unstable angina, or crescendo transient ischaemic attack should perhaps begin for the first few days with a daily dose of at least 160 mg (as in the ISIS-2 trial43 or even about 300 mg.432
Aspirin regimens
The randomised evidence now available for comparing the effects of different antiplatelet regimens on the incidence of vascular events includes not only the trials in figures 8 and 9 but also five, more recent, major trials of aspirin (SALT,277 SAPAT,279 ETDRS,282 Dutch TIA,284 and EAFT293, the results of which are given in appendices 1 and 2. These increase from 3000 to 6000 the total number in figure 9 of high risk patients in trials of less than 160 mg aspirin daily. A total of 5000 of these patients were in trials of exactly 75 mg/day, and among them there was a very definite reduction in vascular events (351/2495 v 470/2517; odds reduction 29% (SD 7%) (2P<0.0001)). Thus as well as the clear evidence in figure 9 that doses of 160-325 mg aspirin daily are effective (odds reduction 28% (SD 3%)), there is now strong evidence that doses of 75-160 mg/day are similarly effective. There is as yet, however, no statistically reliable trial evidence about the main effects of much lower doses. Indeed, in the only major trial that directly compares these lower doses with higher doses284 the results for vascular events were compatible with a difference of 10-15% in either direction (appendix 2).
With respect to much higher doses, figures 8 and 9 suggest that doses of about 1000 mg/day (that is, at least 10 times more than is needed to inhibit cyclooxygenase dependent platelet aggregation), which were widely studied in the earlier trials, are no more effective than the “medium” doses of 75-325 mg/day that have now been more widely studied. It has been suggested that only for patients with a prior stroke or transient ischaemic attack433 doses as high as 1000 mg/day may be preferable, although the trials provide little evidence for this. Even if attention were restricted just to patients with such cerebrovascular disease (including those in the recently reported SALT trial of 75 mg aspirin daily; appendix 1) there would be no significant difference between the protective effects of medium and of high doses of aspirin. However, the amount of evidence just on cerebrovascular patients in aspirin trials is too limited for further subdivision of it into different aspirin regimens to be reliably informative. More important, in the unrestricted analyses in figures 2, 4, and 7 (and 9) there is approximate homogeneity of the effects of antiplatelet therapy, indicating that evidence from different types of patients can and should be combined. Hence it is neither necessary nor appropriate to review the evidence on aspirin dosage from cerebrovascular patients independently of that from other high risk patients.
Other antiplatelet regimens
After aspirin alone, the three most widely studied antiplatelet regimens in these trials were aspirin plus dipyridamole in combination, sulphinpyrazone, and ticlopidine. Significant reductions in vascular events were seen with each of these. But neither the directly randomised comparisons of them against aspirin alone (fig 8) nor the indirect comparisons between the trials of them versus control and the trials of aspirin versus control (fig 9) provided clear evidence of any greater or lesser effects with regimens based on these other drugs than with regimens based on aspirin alone.
Implications
Medium dose aspirin (75-325 mg/day) is now the most widely tested antiplatelet regimen and hence has the most extensive evidence of benefit among high risk patients. No other drug regimen in these trials has been shown to be significantly more effective than aspirin alone (figs 8, 9), and the protective effects of aspirin seem to be at least as great with medium doses as with higher and hence more gastrotoxic424 doses (fig 8, 9). At present, therefore, on grounds of convenience and proved efficacy a medium dose aspirin regimen might be a reasonable first choice for patients who need routine antiplatelet therapy, except for the small minority with a clear contraindication to aspirin (for example, definite allergy or severe gastric symptoms even with medium dose enteric coated formulations). For these, some other antiplatelet drug (for example, ticlopidine) might be more appropriate.
The lack of any statistically significant differences between various antiplatelet regimens does not necessarily mean that those regimens are exactly equivalent. For example, although the direct comparisons of aspirin plus dipyridamole versus aspirin alone indicated that dipyridamole produces no worth-while additional reduction in vascular events (316/2661 with aspirin plus dipyridamole v 312/2656 with aspirin alone; fig 8), it does not prove this. Similarly, although the direct comparisons of ticlopidine versus aspirin are non-significantly favourable to ticlopidine, the results are consistent with ticlopidine being either a little better or a little worse than aspirin. But figures 8 and 9 suggest that if there are real differences between one antiplatelet regimen and another in their effects on vascular events, then these differences are unlikely to be large. If, therefore, antiplatelet regimens are to be shown to differ from each other then direct randomised comparisons may be needed that are (in aggregate) of sufficient size, with a total of a few thousand vascular events, to detect the sort of moderate additional effects (perhaps involving odds reductions of only about 10% or, at most, 20%) that could realistically be hoped for in comparisons of other antiplatelet treatments against 75-325 mg aspirin daily.
Optimal Duration Of Antiplatelet Treatment
It is difficult to determine directly from the trials how long antiplatelet therapy should be continued, as there are as yet no large directly randomised comparisons of different durations of treatment. For those trials among patients with a history of myocardial infarction, stroke, or transient ischaemic attack that provided individual patient data, information was available on events occurring during the first, second, and subsequent years of the scheduled treatment period. There was an apparent pattern (figs 10, 11), of a greater effect during the earlier years which superficially suggested that the additional effects of antiplatelet therapy become smaller as treatment is continued. There are, however, difficulties in interpreting such patterns.
Firstly, as time goes by, non-compliance with allocated treatment (that is, stopping antiplatelet therapy in the treatment group and starting it in the control group, perhaps when non-fatal events occur) tends to increase so that any underestimation of the effects of actually using treatment provided by these “intention to treat” analyses tends to be more serious during later years (see below). Secondly, patients remaining at risk of a first event in the treatment group include some who would, in the absence of treatment, already have suffered a vascular event, biasing the comparisons in later years. In the absence of evidence to the contrary from some extensive direct randomised comparisons of different durations of antiplatelet therapy, therefore, it may be prudent to consider indefinite continuation of antiplatelet therapy in patients who remain at high risk of occlusive vascular events, unless some clear contraindication develops.
Size Of Reductions In Risk Produced By Therapy
Figure 11 illustrates the results of the intention to treat analyses that have, to avoid bias, been used throughout this overview. But because there is likely to be some non-compliance in both treatment and control groups in large trials, these analyses slightly underestimate the size of the effect produced by actually taking antiplatelet treatment. This is true for non-fatal events (such as the first non-fatal myocardial infarction or non-fatal stroke during the trial) that are typically of sudden onset, but it may be even more true for vascular death, as death may be preceded by some illness that results in deviations from the allocated trial treatment. Indeed, in some studies the occurrence of a non-fatal vascular event was to be a reason for stopping trial medication. Conversely, control patients thought to be at some particular risk of death, perhaps because they have suffered a non-fatal vascular event, may start taking antiplatelet treatment. In the main trials of prolonged antiplatelet therapy among patients with a history of prior myocardial infarction, stroke, or transient ischaemic attack the average compliance one year after randomisation appeared to have been no more than 80% (and in the months just before a vascular death it may well have been even less).1 Hence the proportional reductions of about 15% in vascular death and 30% in non-fatal vascular events observed in these trials may reflect proportional reductions of about 20% and 35% respectively with actual use of antiplatelet therapy.
From a medical viewpoint what chiefly matters is not the proportional reduction in risk but the absolute reduction in risk. The results of the overview suggest that, at least among patients at particular risk of occlusive vascular disease (but possibly not in primary prevention among healthy subjects), the proportional risk reductions may be roughly similar in different categories of patients. Consequently, in estimating the absolute reduction in risk likely to be produced by antiplatelet therapy what matters most may not be whether the proportional reduction in vascular death is 15% or 20% but whether the absolute risk is “high” or “low.” In patients at particularly high risk of vascular events the benefits of the actual use of antiplatelet therapy are large. For example, among 1000 patients with acute myocardial infarction about 40 vascular events would typically be prevented during the first month and about a further 40 would be prevented in the next couple of years. And similar sized benefits are likely to be seen with prolonged antiplatelet therapy after stroke or transient ischaemic attack.
Even in a patient population at intermediate risk (such as patients with a history of stable angina, other cardiac disease, atrial fibrillation, or peripheral vascular disease), with “only” about a 5% risk of vascular death and an additional 5% risk of a non-fatal vascular event during two years of treatment, antiplatelet therapy would be expected to prevent about 10 deaths and 20 non-fatal events for every 1000 such patients treated. These benefits, which are now extraordinarily definitely established, compare very favourably to those of other treatments that are currently in wide use. Hence unless some specific contraindication exists, antiplatelet therapy should be considered routinely for all patients whose medical history implies a significant risk of occlusive vascular disease over the next few months or years.
Since the inception of this collaboration several years ago, staff and computing have been provided for the clinical secretariat in Edinburgh by grants from the Medical Research Council (United Kingdom), the Chest, Heart, and Stroke Association (United Kingdom and Scotland), and Edinburgh University (Sir Stanley and Lady Davidson Fund); and for the statistical secretariat by the Clinical Trial Service Unit (Nuffield Department of Clinical Medicine, University of Oxford), which is supported by the Medical Research Council, the British Heart Foundation, and the Imperial Cancer Research Fund, and by a Harvard visiting professorship for R Peto. In addition, support was provided (in ignorance of the final results) by Boehringer Ingelheim (UK), Ciba Geigy (USA), EISAI (Europe), European Aspirin Foundation, Glaxo (UK), Glenbrook Laboratories Division of Sterling Drugs (USA), ICI (UK), Lilly (UK), Reckitt and Colman (UK), and Sanofi (Europe).
Collaborators
Argentina: R Altman, L Carreras, R Diaz, E Figueroa, E Paolasso, J C Parodi. Australia: J F Cade, G Donnan, M J Eadie, T P Gavaghan, E F O'Sullivan, D Parkin, J T G Renny, C Silagy. Austria: H Vinazzer, F Zekert. Belgium: H Adriaensen, J M Bertrand-Hardy, M Bran, J L David, J Dricot, E Lavenne-Pardonge, R Limet, A Lowenthal, M Moriau, S Schapira, P Smets, J Symoens (deceased), R Verhaeghe, M Verstraete. Brazil: A Atallah. Canada: H Barnett, R Batista, J Blakely, J A Cairns, R Cote, J Crouch, G Evans, J M Findlay, M Gent, Y Langlois, J Leclerc, J Norris, G F Pineo, P J Powers, R Roberts, L Schwartz, J Sicurella, W Taylor, P Theroux, A G Turpie, R D Weisel. China: J Cui, L Liu. Czechoslovakia: J Pirk. Denmark: C Bay, G Boysen, J B Knudsen, P Petersen, P S Sorensen, H K Tonnesen, Finland: P T Harjola. France: J C Arcan, B Balkau, J Blanchard, J-P Boissel, B Boneu, M G Bousser, M Brochier, M Cloarec, G Cribier, M Dechavanne, P Drouin, E Eschwege, B Guiraud-Chaumeil, R Hugonot, A Leizorovicz, Y Loria, L Michat, J Mirouze, E Panak, J Pasteyer, A Rascol, L Revol, M Roy, J Selles, G Slama, C Starkman, M Teule, N Thibult, M Verry. Germany: F W Albert, K Andrassy, K Breddin, R Eckel, A Encke, J Frohlich, B Hartung, H W Heiss, H Hess, B Hofling, D Krause, G Latta, H Linke, D Loew, R Lorenz, K Middleton, G Novak, M Oldendorf, N Pfluger, D Raithel, R Reuter, G Schettler, J Schnitker, W Schoop, H Stiegler, K Uberla, G Vogel, M Weber, I Welbers, E Zeitler. Greece: G Arapakis. Hong Kong: T Chan, C K Mok. Hungary: R Szabo. India: N P Misra, K Reddy. Ireland: G A FitzGerald. Italy: A Apollonio, F Balsano, A Basellini, L Candelise, M Catalano, N Ciavarella, G Ciuffetti, S Coccheri, M Cortellaro, G Corvi, V Coto, G Davi, R De Caterina, T Diperri, C Fieschi, R Gentile, L Gregoratti, P Gresele, M Lavezzari, A Libretti, B Magnani, G Nenci, G Pagano, C Patrono, L Pedrini, M Pini, Prandoni, F Romeo, F Rovelli, G Rudelli, G Ruvolo, G P Signorini, G Tognoni, F Violi. Japan: T Fujimori, M Kageyama, T Katsumura, S Kitamura, K Maeda, A Suzuki, H Tohgi, S Uchiyama, H Utsumi. Mexico: A M Garcia. Netherlands: A Algra, G J H Den Ottolander, A J Funke Kupper, J van Gijn, H Hart, L J Kappelle, P J Koudstaal, T Lemmens, J Lodder, M Pannebakker, P W Serruys, A Van den Belt, J Van der Meer, A B Van der Vijgh, F W A Verheugt, G Veth. Norway: J Dale, K-A Johannessen, E Thaulow. Romania: P Popescu, N Tiberiu. Spain: J R Domenech Aznar, E Esmatjes, P Guiteras, J Lasierra, P Lopez-Trigo, A Oriol, L Pomar, E Rocha, F de la Gala Sanchez, J Sancho-Rieger, G Sanz. Sweden: U L F Berglund, C Blomstrand, M Boberg, M Britton, C-E Elwin, C Helmers, J Holm, L Janzon, S Juul-Moller, H Mulec, J E Olsson, S Persson, G Rasmanis, A Rosen, K Samuelsson, J Soreff, N Wahlgren, L Wallentin. Switzerland: H R Baur, M Bokslag, A Bollinger, B Meier, M Pfisterer, N Pfluger. Thailand: C Sitthi-Amorn. United Kingdom: E J Acheson, P Appleby (secretariat), A W Asscher, A Aukland, C Baigent (secretariat), S Bala, A H Barnett, P Bell (secretariat), S Bews, G V R Born, J P Branagan, N Brooks, M J Brown, N L Browse, R Capildeo, M Carmalt, A E Carter, I Chalmers, M Clarke, R J Clarke, C A C Clyne, R Collins (secretariat), E D Cooke, G Coutts, D H Cove, P S Crowther, W F Cuthbertson, D De Bono, C Dickerson, J P Dickinson, R Doll, J A Dormandy, D Dunbabin (secretariat), S Ell, P Elphinstone (secretariat), P Elwood, V Englishby, B Farrell (secretariat), C Fiskerstrand, M Flather, T Foley, T Foulds, K M Fox, P Franks, H Fraser (secretariat), T Gardecki, M Gawel, A E Gent, A H Gershlick, J Godwin (secretariat), M Goldman, C Gray, D Gray, R Gray, H Handoll (secretariat), G Hankey, M J G Harrison, N Henderson, S Heptinstall, S F Hobbiger, E W Jones, N A G Jones, S Jost, D Julian, J Kellett, R C Kester, G Lowe, J Mackenzie (secretariat), C N McCollum, G Mead (secretariat), T W Meade, D Mendelow, J C Miller, G K Morris, C Nichol, M Noble, J R O'Brien, M Ogier (secretariat), S Parish (secretariat), M J Parry, R Peto (secretariat), J Powell, P Pozzilli, N Qizilbash, A Rahman, S M Rajah, D H Richards, S Richards, R Ripley (secretariat), V C Roberts, F C Rose, R W Ross Russell, P C Rubin, C V Ruckley, P Sandercock (secretariat), M D M Shaw, K M Shaw, J H Shelley, J Slattery (secretariat), P Sleight, S J Smith, P Stewart-Long, P M Sweetnam, M J B Tansey, H Tindall, J Turney, H M Tyler, N C Varey, M P Vessey, M G Walker, M A Walker, C P Warlow (secretariat), R G Wilcox, H Willems, E H Wood, E Wyn-Jones. United States: H P Adams, B Barton, R F Bedford, B L Bick, S Bingham, B G Brown, T Bryant, J Buring, C F Cabot, P Canner, J Chesebro, O D Chrisman, G P Clagett, J A Colwell, M Dyken, D Ellis, W S Fields, C Furberg, V Fuster, S Goldman, J Granett, R M Green, D Green, R Hardy, L A Harker, W H Harris, R G Hart, W K Hass, C Hennekens, D Hill, M Hume, M C Igloe, G Johnson, S Jonas, G Knatterud, T R Kohler, N J Lembo, D Lewis, E Lockhart, P Majerus, M T McEnany, R McKenna, J L Mehta, J S Meyer, B Molony, T Moritz, D M Nicoloff, G Nycz, H Ono, G A Pantely, S J Phillips, P Ridker, J T Robertson, R Rothbart, E W Salzman, R D Sautter, R C Schlant, J A Schoenberger, M V Sengekontacket, G Sharma, P Steele, K P Steinnagel, J Stratton, J M Sullivan, G Timmis, J F Toole, M D Walker, S Weisman, C W White, M Wirecki, D Wombolt, R Wong, S Yusuf, K Zadina, D Zucker.
Writing Committee
Oxford: R Collins, R Peto, C Baigent. Edinburgh: P Sandercock, D Dunbabin, C Warlow.
Individual results of unconfounded randomised comparisons of prolonged antiplatelet therapy (scheduled duration one month or more) with control (A upsilion C)
Unconfounded randomised trials comparing one prolonged antiplatelet regimen with another (A1 upsilon A2)